
Active participation in social care means helping a person take part in their own care, support, and daily life as far as they can and want to. Staff do not simply do tasks for someone and move on. They work with the person, not around them. That idea sits close to person centred care, where support is built around the individual’s choices, routines, values, and goals.
This approach treats the person as an active part of their own life, not as someone who just receives help. They may want to choose what time they get up, how they spend their day, what food they eat, who supports them, or how personal care is given. Those choices are not small. They shape dignity, comfort, confidence, and identity. Regulation 9 on person centred care and CQC guidance on independence, choice and control both reflect that wider picture.
“Active participation turns care from a task list into a shared process.”
Active participation can look different from one person to the next. For one person, it may mean choosing clothes and deciding how to spend the afternoon. For another, it may mean helping shape a care plan, keeping hold of part of a daily routine, or staying involved in community life. The detail changes. The principle stays the same. The person should be involved in real ways that fit their abilities, communication style, and wishes.
That is also why this idea goes beyond offering quick choices that sound polite but change nothing. A rushed question asked with no real option behind it is not participation. A person needs time, information, and support to take part properly. Skills for Care’s work on independence, choice and control points in the same direction, and NHS England’s overview of personalised care shows how choice and control are tied to better care experiences.
A person may not do every part of a task alone. Still, they may do part of it with support, extra time, adapted equipment, or clear communication. Someone with arthritis may wash and dress themselves with aids. Someone living with dementia may still show preferences through gestures, tone, or routine. Someone with a learning disability may need information broken down more clearly before making a choice. Participation is not about pushing independence too far. It is about not taking over when support could keep the person involved.
Why active participation affects wellbeing and outcomes
When people are involved in their own care, they often feel more respected and more like themselves. Care can easily become something that strips away confidence if staff rush, assume, or decide everything in advance. By contrast, when a person is asked, listened to, and included, they are more likely to feel seen as an individual. That can protect self esteem at a time when illness, disability, frailty, or life changes may already be making life feel smaller.
“Being involved helps people keep hold of who they are, not just what support they need.”
There is also a practical side. People often keep skills for longer when they continue to use them. That may include washing, dressing, eating, moving about, making choices, or joining conversations. If staff take over too quickly, those skills can weaken. Confidence can drop with them. NICE guidance on patient experience notes that many people want to be active participants in their care, and the same thinking applies in social care settings where daily support shapes everyday life.
This approach also supports identity. A person is rarely defined by a care need alone. They may still see themselves as a parent, friend, gardener, volunteer, cook, neighbour, or member of a faith group. Good care should leave room for those roles. Meanwhile, support that focuses only on tasks can keep someone physically safe while leaving them detached from the parts of life that give them purpose.
There is a common counterpoint here. Some people argue that active participation takes too much time, especially in busy services. There is some truth in that. It can take longer to support someone to do part of a task than to do it all for them. Yet that short term saving often leads to more dependence later. Staff may then need to provide more support, not less. On second thought, the issue is not simply time. It is what sort of care that time produces.
For staff, this changes the job. Good support is not only about finishing tasks safely. It is also about noticing what the person can still do, what they would like to do, and what support would help them stay involved. The Care Certificate standard on person centred working reflects that way of thinking. So does shared decision making guidance from NHS England, which shows how better outcomes often start with better conversations.
What active participation looks like in day to day care
Active participation makes the most sense when it is tied to ordinary parts of daily life. In personal care, a person may choose when they wash, which products they use, or which parts of the task they want to do themselves. At mealtimes, they may choose food, help prepare it, or use equipment that supports independent eating. With mobility, staff may encourage the person to transfer with guidance rather than lifting them straight away, where that is suitable and safe.
Communication runs through all of this. A person cannot take part properly if information is given in a way they cannot follow. Some people need plain language. Some need visual prompts, signing, objects, repetition, hearing support, or more time. Others may show choice through facial expression, movement, behaviour, or routine rather than speech. NICE guidance on shared decision making and NHS England’s decision support tools page both point to the value of presenting options clearly and in a way the person can use.

“Participation is not reserved for confident speakers. It includes anyone whose life is shaped by care.”
Examples help. So do small details.
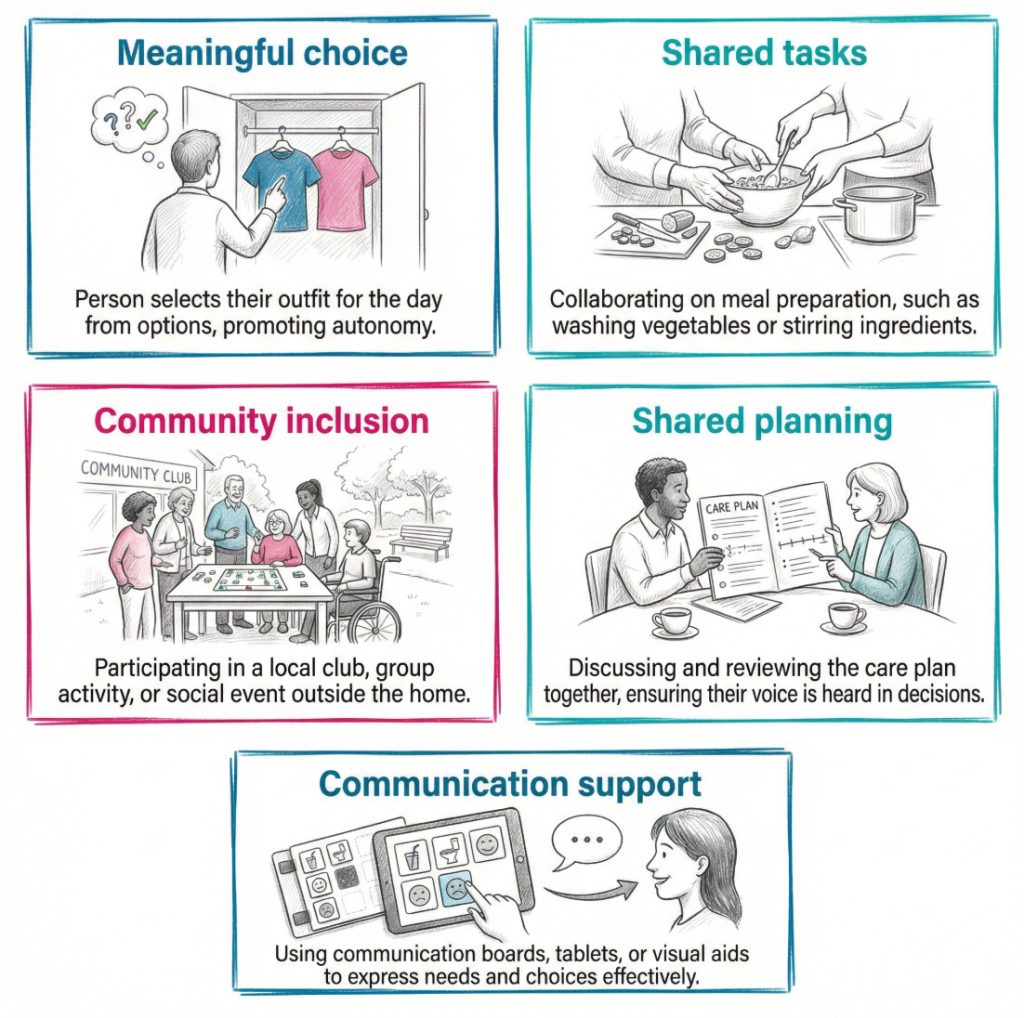
- Daily routines: A person chooses when to get up, what to wear, and how their room is arranged. These everyday choices help preserve identity and stop care becoming routine led.
- Personal care: The person washes their face, chooses toiletries, or decides the order of support. This keeps a sense of privacy and ownership over intimate care.
- Meals and drinks: The person picks what they want, helps prepare part of a meal, or eats with adapted equipment. This supports both independence and enjoyment.
- Care planning: The person helps review what is working, what is not, and what goals they want to keep or change. That makes the plan more personal and more realistic.
- Relationships and community life: Staff support contact with family, friends, faith groups, clubs, or familiar places. This can reduce isolation and help the person stay connected to the life they value.
- Shared tasks: The person folds clothes, waters plants, sets the table, or chooses music. These are simple actions, yet they can carry a strong sense of purpose.
A brief example makes the point. An older person in residential care may need help with dressing because of stiffness and pain. One approach is for staff to dress them quickly every morning. Another is to lay out two outfits, give enough time, support the buttons, and let the person do the rest. The second approach may take longer. It also protects choice, movement, and confidence.
A caveat here is that participation should not be forced. Some days a person may be tired, distressed, unwell, or simply not want to do as much. Respect includes recognising that choice as well. Staff need to notice the difference between encouraging involvement and pushing someone past what feels right for them.
Barriers to active participation and the role of staff
Active participation can be hard to maintain when barriers build up. Some sit with the person’s circumstances. Pain, fatigue, memory loss, low mood, confusion, reduced confidence, sensory loss, and poor past experiences can all make involvement harder. Some barriers come from the service itself. Short staffing, time pressure, fixed routines, poor communication, or a culture that leans too heavily on risk avoidance can all narrow the person’s role in their own care.
Assumptions cause trouble too. Staff may assume that because someone needs support in one area, they cannot do much in another. They may take silence as agreement. They may mistake slow responses for a lack of ability. They may see behaviour as a problem rather than a form of communication. Those habits can shut people out very quickly. CQC guidance on treating people as individuals stresses the need to know the person properly rather than rely on labels or routine.
“The biggest barrier is often not incapacity. It is assumption.”
Staff responsibilities follow from that. Good care depends on noticing strengths as well as needs and adjusting support so the person has a fair chance to join in.
- Observe strengths: Staff should look for what the person can still do, not only what they struggle with. That makes support more balanced and less restrictive.
- Adapt the approach: Staff may need to change pace, timing, language, equipment, or the setting. Small changes can open the door to much more involvement.
- Balance safety with autonomy: Support should reduce avoidable harm without removing choice altogether. A person can rarely feel dignified if every decision is made for them.
- Review routine honestly: Teams should notice when convenience has started to replace involvement. That sort of reflection often shows where care has become task centred.
- Work with the wider circle: Family, friends, and advocates can help explain preferences, routines, and ways of communicating. Their role should support the person’s voice, not replace it.
A short case example helps here too. A man with dementia may stop joining mealtimes and start wandering instead. Staff might read this as refusal and serve meals separately. Another reading is possible. The dining room may be noisy, crowded, and confusing. A quieter seat, a familiar plate, visual prompts, and support from the same worker may help him stay involved. Same person. Different response.
Still, staff also have to think about risk. Some tasks do carry hazards. Moving about, preparing hot drinks, or taking part in household activities may need support and judgement. Good care does not remove all risk from life. It looks for proportion. Skills for Care’s person centred care resources and NICE guidance on social work with adults experiencing complex needs both support fuller involvement in decisions, even when support needs are significant.
How active participation links with person centred care, dignity, and rights
Active participation is one of the clearest signs that care is person centred. A service may say the right words. The real test is whether the person can shape what happens to them day by day. Their care plan should reflect their physical, emotional, mental, social, and cultural needs. Their preferences should be known by staff. Their choices should affect how support is given. CQC’s person centred care guidance sets out that broader view clearly.
Dignity is tied to this as well. Dignity is not just about polite language or knocking on doors. It is also about control, privacy, and whether the person’s wishes carry real weight. Someone receiving intimate care can feel exposed very quickly if staff rush or take over. By contrast, when the person chooses how support is given and takes part in parts of the task they want to keep, the whole experience changes. It feels less like something done to them.
This also links to rights and inclusion. People who use services should not see their lives shrink to meals, medication, and personal care. They may still want education, employment, volunteering, faith, hobbies, friendship, family contact, and a place in their community. Social care should support that wider life where possible. Personalised care from NHS England describes a shift in power and decision making, and that shift sits at the heart of active participation.
Meanwhile, there is a practical lesson for staff and learners. Active participation is both a value and a method. It is a value because it shows respect for the person. It is a method because it changes conversations, care planning, reviews, activities, routines, and everyday support. After all, the best question in social care is often very simple: what can this person still do, and how can support help them keep doing it?
A short checklist can help test whether active participation is really happening.
- Choice is genuine: The person is offered real options, not a token question with one likely answer.
- Information is clear: The person receives information in a way they can understand and respond to.
- Support fits the person: Staff adjust pace, language, timing, and equipment to help the person join in.
- Daily life stays personal: Routines reflect the individual’s preferences, habits, and relationships.
- Skills are maintained where possible: Staff avoid taking over when guided support would keep the person involved.
- Community links are protected: The person is supported to stay connected to people and places that mean something to them.
- Reviews include the person: Care plans are shaped with the person, not simply written about them.
Conclusion and next step
Active participation in social care means more than offering choice now and then. It means helping people stay involved in their own lives, their own routines, and their own care. When that happens, care feels more respectful, more personal, and more human. It can support confidence, preserve skills, and protect dignity at the same time.
The opposite is easy to slip into. Staff get busy. Tasks stack up. Routines harden. People are helped in ways that gradually leave them with less say and less control. That is why active participation deserves close attention in training, supervision, care planning, and day to day practice. Small decisions. Real consequences.
For staff, the next step is usually reflection rather than a new form or policy. Look at ordinary support. Washing, dressing, meals, moving about, activities, reviews, visits, and conversations. Ask where the person is genuinely involved and where care has become too task focused. That question often shows what needs to change.
Active Participation FAQ
What does “active participation” mean in the context of adult social care?
A: Active participation means that individuals receiving care are involved in making decisions about their care and support. They have a say in the planning, delivery, and evaluation of their care, ensuring that their preferences and needs are respected.
How can service users become active participants in their care?
A: Service users can become active participants by engaging in the creation and review of their care plans, expressing their preferences and choices, providing feedback on services, and participating in meetings or forums where they can discuss their care.
What are the benefits of active participation in adult social care?
A: The benefits include greater satisfaction with care services, enhanced well-being, improved quality of life, increased autonomy, and a sense of empowerment. It also leads to more tailored and effective care delivery.
What role do care providers play in promoting active participation?
A: Care providers support active participation by creating an inclusive environment, providing relevant information, encouraging feedback, involving service users in decision-making processes, and respecting their choices and preferences.
Can family members be involved in active participation?
A: Yes, family members can be involved if the service user wishes. They can participate in care planning, provide support, and advocate for their loved one’s needs and preferences.
What if a service user has difficulty communicating their needs?
A: For service users who have difficulty communicating, advocacy services can help. Advocates represent the service user’s interests and ensure their voice is heard in care planning and decision-making processes.
How can feedback from service users drive improvements in care services?
A: Feedback from service users provides valuable insights into their experiences and needs. Care providers can use this feedback to make necessary adjustments and improvements to services, ensuring they are more responsive and effective.
Are there any legal frameworks supporting active participation in adult social care?
A: Yes, the Care Act 2014 is a major legal framework that supports active participation. It emphasises well-being, personal dignity, choice, and control as fundamental principles in adult social care.
What resources are available for individuals who want to be more actively involved in their care?
A: Resources include advocacy services, care planning tools, training sessions, informational booklets, and support groups. Local authorities and care providers often offer these resources to help individuals become more engaged in their care.
How can technology facilitate active participation in adult social care?
A: Technology can facilitate active participation by providing tools like care apps, virtual health monitoring, and online forums for communication with care teams. These tools enable service users to take a more proactive role in managing their health and care.
What are some examples of activities that promote active participation in care homes?
A: Examples include residents’ meetings to discuss care and activities, involvement in menu planning, organising social events, and taking part in the recruitment process for new staff members.
How does active participation contribute to a person-centred approach in adult social care?
A: Active participation ensures that the care delivered is personalised and aligned with the individual’s unique needs, preferences, and goals. It places the individual at the centre of their care, fostering a more compassionate and responsive care environment.
What challenges might be encountered in fostering active participation, and how can they be addressed?
A: Challenges may include communication barriers, lack of awareness, and resistance to change. Addressing these challenges involves providing accessible information, using communication aids, offering training, and fostering a culture that values and respects service user input.
Can service users opt out of active participation?
A: Yes, active participation is a choice, and service users can opt out if they prefer. However, care providers should make every effort to encourage and facilitate participation while respecting the individual’s wishes.
How do care providers ensure that active participation is meaningful and not just a tick-box exercise?
A: Care providers ensure meaningful participation by genuinely listening to service users, taking their feedback seriously, making real changes based on input, and involving them in every stage of care planning and delivery. They should also provide regular updates on how service user feedback has been implemented.
If you have further questions or specific concerns regarding active participation in adult social care, please reach out to your local care provider or advocacy service for personalised assistance.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.