
Summary
- Barriers Impacting Access: Health and social care professionals face various obstacles, including physical, economic, and cultural barriers that hinder access to services and affect care quality.
- Physical and Economic Challenges: Geographic isolation, high healthcare costs, and inadequate infrastructure contribute to difficulties in accessing necessary treatment, particularly for those in rural areas.
- Cultural and Systemic Issues: Language barriers and cultural beliefs can prevent effective communication and care. Bureaucratic complexities often frustrate both patients and providers, leading to fragmented services.
- Strategies for Improvement: Enhancing accessibility through better infrastructure, improving affordability with financial assistance, promoting cultural competence, and streamlining systems are essential steps to create a more equitable health and social care environment.
A barrier in health and social care is anything that blocks, delays, or weakens a person’s access to support. Sometimes it is obvious. A building may have steps, a website may not work with screen readers, or a letter may be packed with technical language. Sometimes it is less visible. A person may feel embarrassed, frightened, rushed, or judged, so they hold back important information or avoid care altogether.
Barriers do not only affect whether someone gets through the door. They shape whether a person feels safe, whether they can follow what is happening, and whether they stay involved in decisions about their own care. That wider picture links closely to the social factors that shape health, such as housing, income, education, disability, transport, and social support. The NHS health literacy resources, the NHS guide to health literacy, and NICE guidance on patient experience all reflect that same idea in different ways.
“A service can be open, staffed, and well intentioned, yet still be hard to use.”
Many barriers are created by the setting rather than by the person. If letters are hard to read, appointments are too rigid, or communication support is missing, the problem does not sit neatly with the individual. The service may be asking people to fit around its systems instead of shaping care around real needs. That can leave people labelled as disengaged when they are actually facing obstacles at every stage.
This changes how barriers should be viewed. They are not side issues. They sit right in the middle of safe, respectful care. Staff need to notice them early, services need to reduce them where they can, and leaders need to look at whether systems are helping or hindering the people who rely on them.
The Main Types of Barriers People May Face
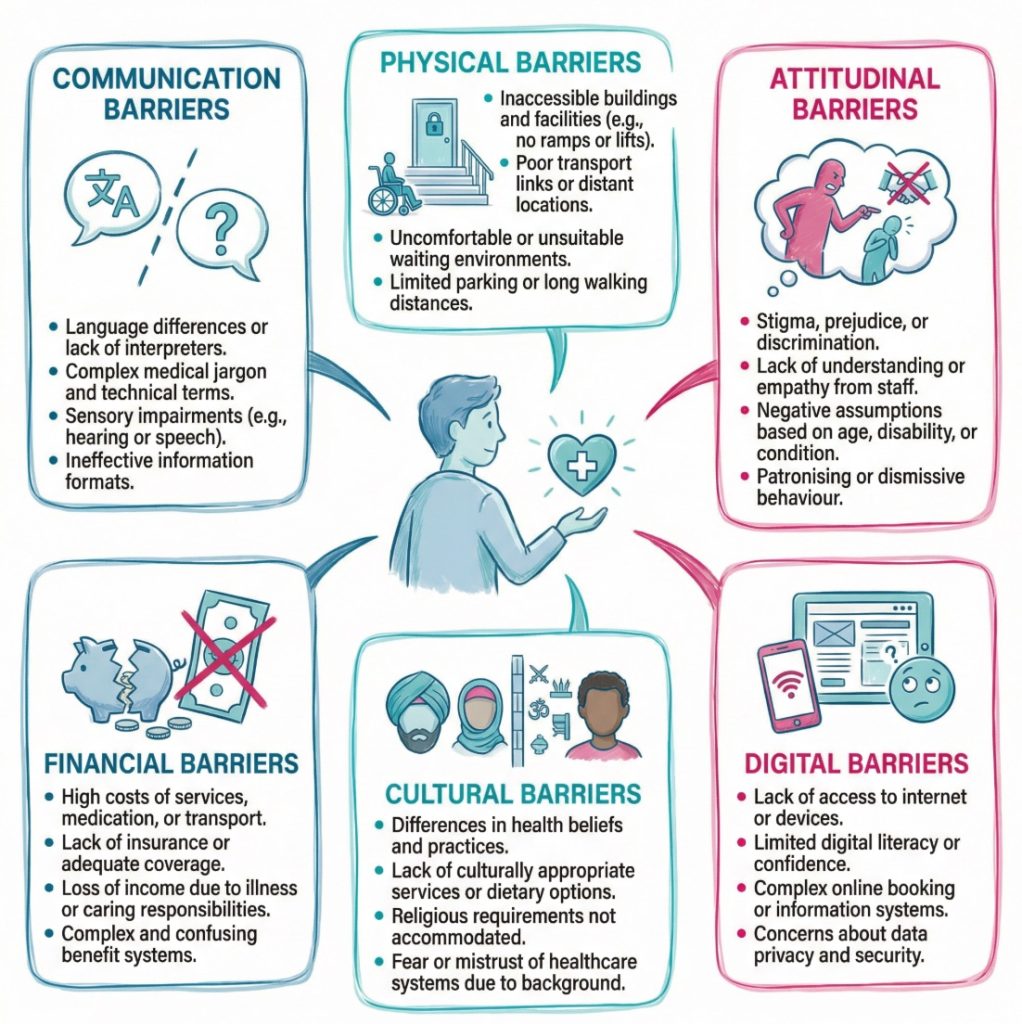
Barriers usually fall into a few broad groups, although real life is rarely neat. Communication barriers are common and can affect every part of care. A person may have limited health literacy, hearing loss, memory problems, a learning disability, or a different first language. Staff may use jargon, speak too quickly, or move on before checking what the person has actually taken in. The Accessible Information Standard and Skills for Care guidance on effective communication both show how communication support shapes safe care.
Physical and environmental barriers are just as important. These include poor building access, unsuitable transport links, weak signage, noisy waiting rooms, inaccessible toilets, or digital systems that do not work with assistive technology. A person may be willing to attend and ready to engage, yet the setting itself may wear them down before any care starts. Meanwhile, digital barriers have become more visible as services rely more on online booking, text reminders, apps, and remote appointments.
Social, emotional, cultural, and financial barriers often sit alongside the others. A person may fear stigma linked to mental ill health, substance use, poverty, sexuality, gender identity, or family circumstances. Someone else may struggle with childcare, travel costs, or time away from work. On second thought, “financial barrier” can sound too narrow here. It is often about the full cost of access, including time, energy, stress, and arranging daily life around a service.
| Barrier type | What it can look like | Effect on care |
|---|---|---|
| Communication | Jargon, rushed speech, hard to read letters, no interpreter | Confusion, poor consent, missed follow up |
| Physical | Steps, poor lighting, narrow doorways, poor signage | Reduced access, lost independence, stress |
| Digital | Online only booking, weak digital skills, inaccessible portals | Missed appointments, exclusion, delay |
| Financial | Travel costs, data costs, unpaid time off work | Late help seeking, cancelled visits |
| Attitudinal | Stereotyping, impatience, low expectations | Loss of trust, reduced choice, poorer experience |
| Cultural and social | Fear of judgement, different beliefs, lack of privacy | Less openness, weaker engagement |
Common examples include:
- Communication barriers: A person may receive letters filled with technical terms or speak with staff who do not pause to check whether the message is clear. This can lead to confusion, weak consent, and poor follow up.
- Physical barriers: Steps, narrow spaces, poor transport, or inaccessible websites can make it harder for people to attend or use services on their own.
- Attitudinal barriers: Stereotypes and low expectations can leave people feeling dismissed, patronised, or ignored.
- Financial barriers: Travel, data, childcare, and lost pay can make care difficult to reach, especially for repeated appointments.
- Cultural barriers: Beliefs about illness, privacy, family roles, or support can affect how comfortable a person feels with services.
“A barrier is often a chain of small obstacles rather than one large problem.”
How Barriers Affect People Receiving Care
Barriers can affect health, safety, independence, and confidence all at once. At the practical level, they can lead to missed appointments, delayed referrals, poor follow through, and avoidable decline. At the personal level, they can leave people feeling shut out. After repeated bad experiences, some stop asking for help until their situation becomes more serious.
Communication barriers show this clearly. If a person does not fully grasp what a professional is saying, they may struggle to describe symptoms, ask questions, or weigh up options. They may agree to something without truly following it. They may also leave with the wrong idea about medicines, tests, follow up, or warning signs. NICE guidance on shared decision making links good care with clear communication and genuine involvement, not just information given once and quickly forgotten.
The emotional effect can be just as heavy. Feeling judged, rushed, or not believed can create anxiety before each contact with a service. Some people then become quieter in appointments. Others miss visits because the whole process feels too hard. Granted, not every missed appointment points to a barrier. People do forget or change their minds. Still, services that look only at attendance figures can miss the wider picture.
Some groups face several barriers at once. An older person with hearing loss may struggle with phone systems, long waits, and confusing written information. A disabled adult on a low income may deal with transport problems, building access issues, and staff assumptions in the same week. A person with low literacy may avoid asking questions because they fear embarrassment. Those combined pressures can widen gaps in access and outcomes over time.
Examples from day to day care include:
- Missed information: A person nods during an appointment but leaves unsure about what happens next. Staff may assume they understood when they did not.
- Reduced choice: A person may accept the only option that feels manageable, rather than the one that best fits their needs.
- Loss of confidence: Repeated poor experiences can make someone stop speaking up or stop seeking help early.
- Greater dependence: When systems are hard to use, people may rely more on relatives or carers just to get basic support arranged.
“When people cannot use a service easily, the result is often silence, delay, or withdrawal.”
Why Barriers Are Also a Staff and Service Issue
It is tempting to describe barriers as personal difficulties. That is too simple. Staff behaviour, service design, and workplace culture all shape whether care feels open or closed to the people using it. A barrier can come from the booking system, the waiting room, the wording of a letter, the lack of interpreter support, or the tone used in an assessment. Because of that, barriers are also a service issue from the start.
Attitudinal barriers deserve close attention. These appear when workers make assumptions about a person because of age, disability, diagnosis, appearance, background, or the way they communicate. Staff may assume an older person will not want detailed information, or that a person with a learning disability cannot make decisions, or that someone who misses appointments simply does not care. Skills for Care examples on listening to and involving people and Skills for Care resources on person centred care both reflect how much difference this makes.
Services can also create barriers by accident. A rigid appointment model may not work for people with fatigue, anxiety, caring roles, or transport difficulties. A digital first system may exclude people who do not have the device, confidence, data, or access needs to use it well. For example, the Accessible Information Standard requirements set out how information and communication needs should be identified, recorded, shared, met, and reviewed. That is not just paperwork. It affects whether care is actually usable.
A common counter point is that services are under pressure and cannot tailor everything for everyone. There is some truth in that. Time is limited, staff are stretched, and systems are often inherited rather than chosen. Yet small changes can prevent larger problems later. A clearer letter, a recorded communication need, a better choice of appointment format, or a quieter explanation can reduce missed contacts, repeat work, distress, and complaints.
Common mistakes that make barriers worse include:
- Assuming understanding: Staff may mistake politeness or silence for clear understanding.
- Using one format only: A service may send all information in the same style, even when people need alternatives.
- Blaming the person too quickly: Non attendance or low engagement may be treated as a personal failing rather than a sign of blocked access.
- Overlooking cumulative pressure: Several modest barriers can combine and have a far bigger effect than any one of them alone.
“Respect is not only about tone. It is also about whether the system makes room for the person.”
Ways Barriers Can Be Reduced in Practice
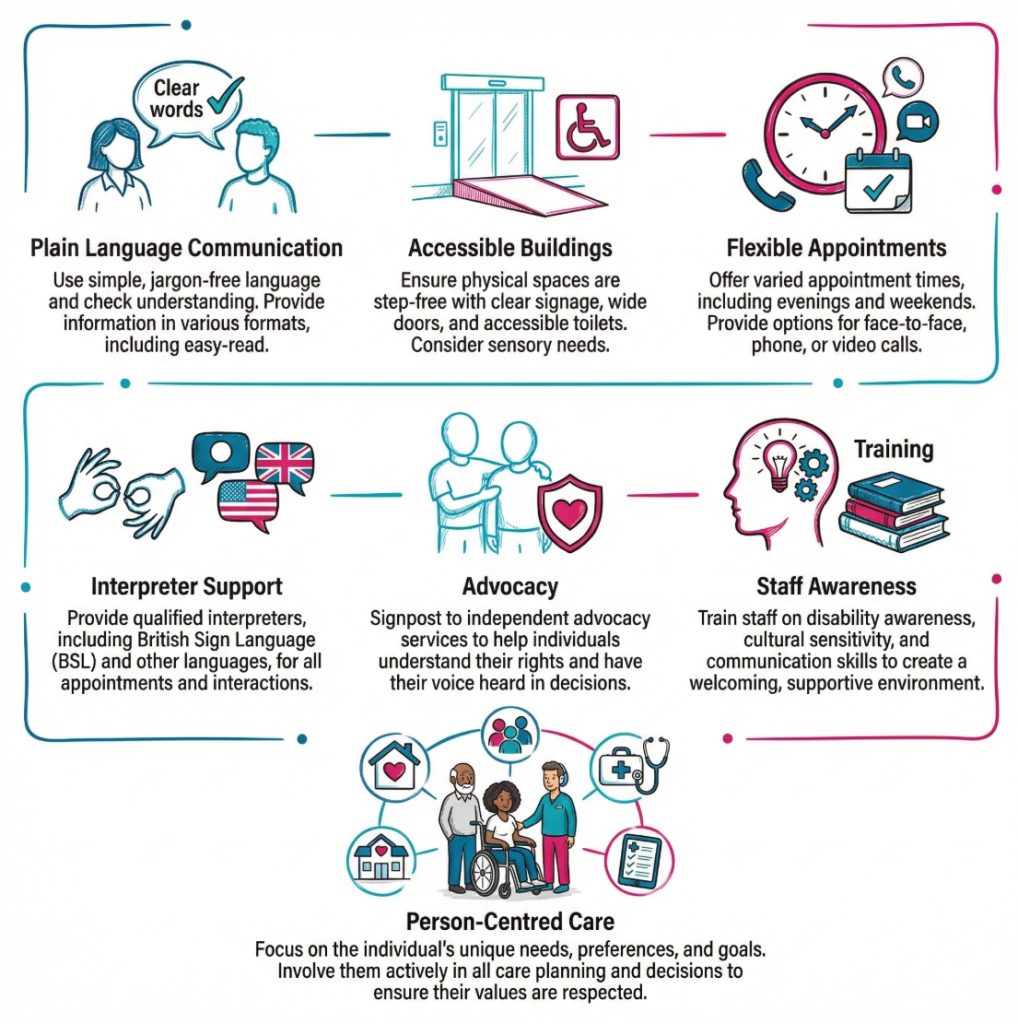
Many barriers can be reduced through steady, practical changes. Person centred care is one of the strongest starting points. It means learning how the person communicates, what support they already use, what causes stress, and what helps them feel involved. Skills for Care on person centred care and NICE patient experience guidance both point in that direction. Put plainly, the same service can feel manageable for one person and unworkable for another.
Clear communication is often the most immediate area for improvement. Staff may need to use plain language, explain unusual terms, slow the pace, and check what the person has taken from the conversation. Easy read information, translated material, large print, Braille, British Sign Language support, and well designed digital content can all help. The NHS easy read health resources, government guidance on accessible communication formats, and the NHS Accessible Information Standard page all support that broad approach.
A simple step by step approach often works best:
- Spot the barrier: Staff notice where the person is struggling, whether that is transport, language, anxiety, digital access, noise, or written information.
- Record the need: The support needed should be noted clearly so it does not rely on memory or chance.
- Adjust the contact: The format, pace, setting, or timing can then be changed to suit the person better.
- Review what happened: The service can check whether the adjustment actually worked and what still needs to change.
Useful actions include:
- Flexible access: Different appointment types, better reminders, and more realistic timing can help people who have caring duties, work pressures, pain, fatigue, or anxiety.
- Accessible environments: Better signage, step free routes, quieter spaces, and seating that suits different needs can reduce stress and improve independence.
- Inclusive communication: Plain English, easy read, interpretation, and recorded communication needs help people take part more fully.
- Joined up working: Sharing accurate information between teams can spare people from repeating the same details again and again.
- Advocacy and support: Some people benefit from extra help to express their views, weigh up options, or stay involved during assessments and reviews.
A short checklist can help services reflect on whether access is real rather than assumed:
- Information: Can people receive information in a format they can read, hear, or use?
- Environment: Can people enter, move through, and wait in the setting with dignity?
- Systems: Can people book, change, and attend appointments without unnecessary obstacles?
- Staff approach: Do workers check understanding and avoid assumptions?
- Review: Are barriers recorded, revisited, and acted on over time?
Final thoughts
Barriers in health and social care are the things that stand between a person and effective support. They may be physical, digital, financial, emotional, cultural, or linked to communication. Often they overlap. What looks like poor engagement from the outside may be a sign that the service is simply hard to use.
Looking at barriers properly changes the whole picture. It shifts attention away from blame and towards access, respect, and realistic support. It also reminds staff that people do not all start from the same point. Some need more flexibility, more explanation, or a different format before they can take part on equal terms.
There is also a wider lesson here. Good care is not only about what is offered. It is about whether the person can reach it, follow it, question it, and use it in daily life. When services reduce barriers, people are more likely to seek help earlier, feel listened to, and stay involved in decisions. That improves experience, and it can improve outcomes too.
The next sensible step for any service is not grand or complicated. It is to look closely at where people get stuck, what patterns keep appearing, and what small changes could remove avoidable obstacles. Sometimes the barrier is in the building. Sometimes it is in the wording. Sometimes it is in the assumption no one noticed. Small things. Big effect.
Glossary and Key Terms
- Accessibility
The ease with which people can reach and use healthcare services. It includes physical access to facilities and the availability of services. - Bureaucracy
The complex administrative processes that can slow down access to care. It often involves many forms and approvals. - Cultural Competence
The ability of healthcare providers to understand and respect diverse cultural backgrounds. This helps in providing better care to all patients. - Discrimination
Unfair treatment of individuals based on characteristics like race, gender, or disability. It can lead to reluctance in seeking care. - Economic Barriers
Financial obstacles that prevent individuals from accessing healthcare. This includes high costs for treatments and medications. - Fragmentation of Services
When health and social care services do not work together effectively. This can result in disjointed care for patients. - Integrated Care Models
Approaches that encourage collaboration between different healthcare providers. This aims to provide a more cohesive experience for patients. - Language Services
Support offered to help patients communicate effectively with healthcare providers. This includes interpreters and translated materials. - Psychological Barriers
Emotional factors that hinder people from seeking care. Fear and anxiety about healthcare experiences can play a significant role. - Stigma
Negative perceptions associated with certain health conditions. Stigma can prevent individuals from seeking necessary help or treatment.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.





