
Communication shapes every part of care. It affects how someone explains pain, asks for help, shows fear, shares preferences, and takes part in decisions. In health and adult social care, communication is not limited to speech. It also includes listening, eye contact, body language, facial expression, gesture, touch used appropriately, written information, and the way staff notice distress or hesitation.
A communication barrier is anything that gets in the way of a clear message. Sometimes the barrier is obvious, such as hearing loss, sight loss, or a language difference. Sometimes it is less visible. Pain, anxiety, confusion, trauma, low literacy, autism, fatigue, a rushed ward, or too much background noise can all interfere. So can poor habits, such as using jargon, finishing people’s sentences, or talking to a relative instead of the person receiving care.
“Good care starts with being understood.”
These barriers affect daily care in very practical ways. A person may not say they are in pain because they cannot find the words. Another may nod politely without following what has been said. A person living with dementia may become distressed because there is too much noise and too much information at once. A person with a learning disability may be given written information that is too dense to use. The Accessible Information Standard reflects this clearly by focusing on accessible information and communication support across services.
Staff carry a clear responsibility here. Care should not depend on the person fitting one fixed style of communication. It should adapt to the person. That could mean choosing a quieter room, speaking more slowly, checking hearing aids, using easier wording, or recording communication preferences in the care plan. Guidance from Skills for Care on communication, Alzheimer’s Society on communicating and dementia, and Mencap on communicating with people with a learning disability all point in the same direction. People need communication that works for them, not for the convenience of the service.
The main barriers to communication and what they look like in care settings
Communication barriers tend to fall into a few broad groups. Physical and sensory barriers are among the most common. Hearing loss can make speech sound blurred, especially in a busy room. Sight loss can make it harder to read faces, signs, written information, or gestures. Breathlessness, pain, fatigue, stroke, Parkinson’s, and the side effects of medicines can also affect how a person speaks, listens, or processes information. With aphasia after stroke, the person may know exactly what they want to say but struggle to speak, read, write, or follow language. The Stroke Association’s page on aphasia is useful background on this.
Meanwhile, cognitive and emotional barriers can be just as disruptive. Dementia, delirium, mental ill health, learning disability, autism, fear, grief, and past trauma may all change how a person receives information or responds to it. A distressed person may only hear part of a sentence. Someone living with dementia may lose the thread of a conversation or rely more on tone and facial expression than on long explanations. The NHS hearing loss information and NICE guidance on hearing loss in adults both show how easily hearing difficulties can affect day to day communication and quality of life.
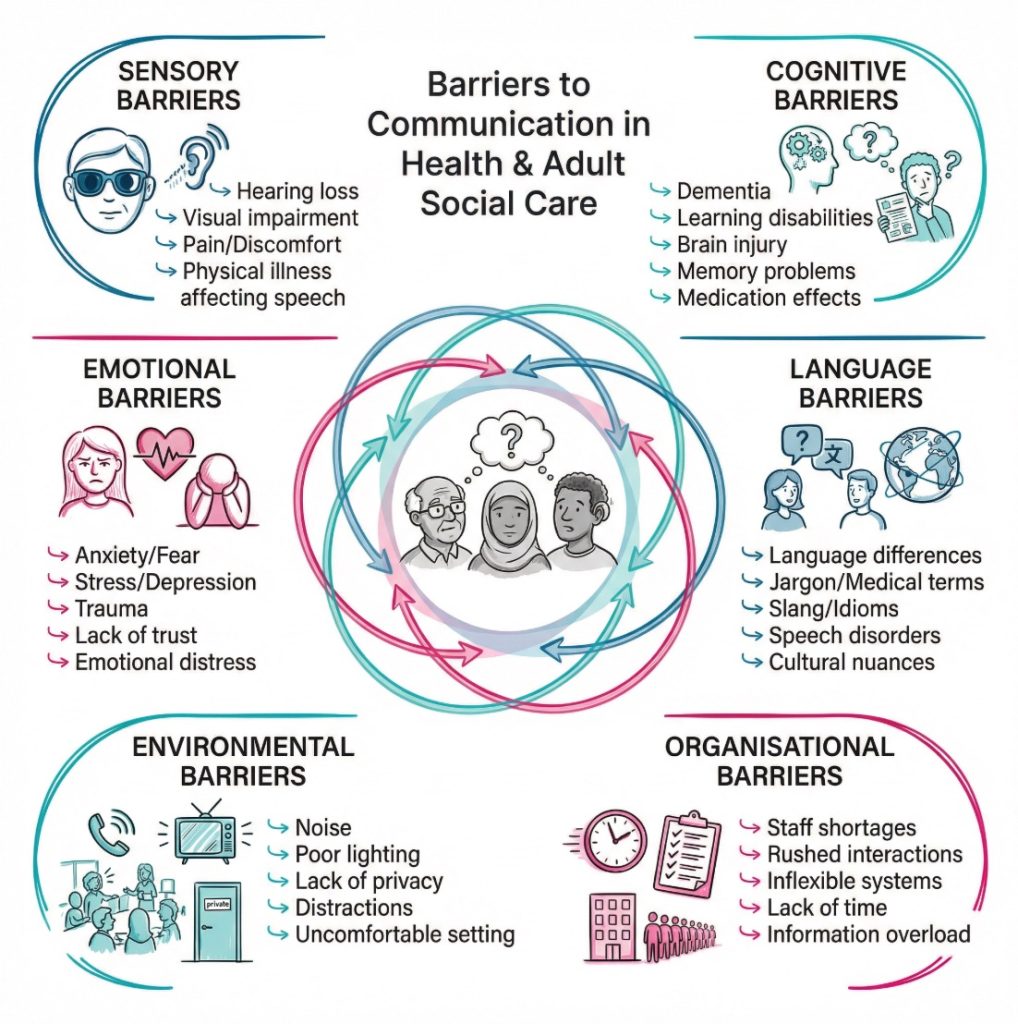
Environmental and organisational barriers often go unnoticed because they seem ordinary. Noise, poor lighting, lack of privacy, interruptions, short appointments, unfamiliar staff, poor handovers, and over reliance on digital systems can all reduce the quality of communication. Attitudes can also become a barrier. Staff may assume someone has understood, speak too quickly, use childish language with adults, or direct all questions to family members. A caveat here is that families can be hugely helpful, especially when they know a person’s routines and signs of distress. Still, the person receiving care should remain at the centre of the conversation wherever possible.
The table below shows how these barriers often present in care settings.
| Barrier type | What it can look like | Likely effect on care |
|---|---|---|
| Sensory | The person misses words, avoids eye contact with bright light, or struggles to read forms | Information is missed, consent may be unclear, distress can increase |
| Physical | Speech is slurred, breathing is laboured, pain limits concentration | Staff may misread need or urgency |
| Cognitive | The person loses track, repeats questions, or cannot process long explanations | Care planning becomes harder and errors are more likely |
| Emotional | Anxiety, fear, anger, shame, or withdrawal affect interaction | The person may stop asking for help |
| Language and literacy | Limited English, jargon, or dense written information blocks access | The person may agree without fully following |
| Environmental | Noise, interruptions, poor lighting, and lack of privacy | Communication becomes rushed and less accurate |
| Organisational | Rotating staff, weak handovers, and poor recording of preferences | Useful information is lost between workers |
“A barrier is not always in the person. It is often in the setting, the pace, or the way information is given.”
How communication barriers affect people receiving care and the staff supporting them
The first effect is often emotional. People may feel ignored, rushed, embarrassed, or spoken down to. Once that happens, trust can drop quickly. They may stop sharing concerns, avoid asking questions, or say yes just to move the interaction along. In adult social care, that can affect almost everything: personal care, food and drink, medication, routines, relationships, and independence. A person who cannot explain hunger, pain, loneliness, or fear may receive support that looks organised on paper but feels poor in real life.
There can also be direct risks. A person may not follow medication advice because the information was unclear. They may miss an appointment because the letter was not accessible. Staff may misread a communication difficulty as confusion, aggression, lack of capacity, or refusal. Granted, staff sometimes work under time pressure and have to make quick decisions. Yet a rushed guess can lead to unfair labels and poorer care. The Accessible Information Standard requirements set out the need to identify, record, flag, share, meet, and review communication support needs for exactly this reason.
For staff, poor communication creates repeated work. Questions have to be asked again. Care plans need correcting. Distress escalates. Small misunderstandings turn into bigger problems. This can also affect teamwork. If one worker discovers that a person responds best to one idea at a time, a visual prompt, or a quiet approach in the morning, that knowledge should travel with the person through handovers and records. Otherwise the next worker starts from the beginning.
On second thought, the biggest impact may not be the delay or the error. It may be the gradual loss of person centred care. When communication is poor, tasks can take over. Washing, dressing, feeding, moving, and documenting get done, but the person’s choices and preferences fade into the background. That is why communication should be treated as part of care itself. Not an optional extra.
A few effects show up again and again:
- Loss of trust: People may stop speaking openly if they feel dismissed or misunderstood. That can hide pain, worry, or safeguarding concerns.
- Reduced safety: Missed information can affect medicines, mobility, consent, and reporting of symptoms. Small gaps can have serious results.
- Less choice: A person cannot make real choices if they do not receive information in a form they can use. Choice becomes superficial.
- More distress: Confusion and frustration can lead to agitation, withdrawal, or refusal. Staff may then respond to the behaviour rather than the cause.
- Inconsistent support: When communication preferences are not recorded, care varies from one worker to the next. That can unsettle the person and slow progress.
Common examples of barriers in real health and adult social care settings
In hospitals and clinics, pace is a common barrier. Staff may be moving quickly between patients, phone calls, screens, and clinical tasks. A person might be in pain, breathless, tired after treatment, or frightened by unfamiliar surroundings. Add hearing loss, limited English, or cognitive impairment, and a short exchange can break down very easily. A nurse asks three questions in a row. The person nods. The conversation moves on. Yet only one question has actually been followed. Too common.
In residential care and home care, routine can become the problem. Staff may know the person well and begin to assume what they want, what they feel, or how they usually respond. Familiarity can help, but it can also narrow attention. Workers may talk through tasks rather than talk with the person. This is often seen during washing, dressing, moving, eating, and medication support. The task is completed, but the person’s voice gets smaller. Resources such as Skills for Care’s communication standard and NHS England’s guidance on meeting the Accessible Information Standard support a more planned and consistent approach.
The examples below show how different barriers can appear in day to day care.
- Sensory loss: An older adult with hearing loss may seem withdrawn during meals or reviews. The real issue may be background noise, poor seating, or staff speaking while walking away.
- Cognitive change: A person living with dementia may become distressed during personal care because instructions are too long, the room is noisy, or staff are unfamiliar. The Alzheimer’s Society guide to communication and dementia explains why calm surroundings and simple phrasing often help.
- Language complexity: A person with a learning disability may agree to a plan they do not fully follow because they want to please staff or do not want to appear confused. The Mencap communication guide highlights the value of clear wording, larger text, and one to one communication.
- Speech and language difficulty: A person with aphasia may know what they need but cannot say it quickly or clearly. The Stroke Association’s aphasia resources show why time, patience, and communication tools can make a big difference.
Mini cases help make this concrete. A man with hearing loss keeps missing parts of ward round conversations because staff speak while looking at the computer screen. He appears passive, but he is actually trying to fill in gaps. A woman with dementia becomes agitated when two carers give instructions at the same time during personal care. She is described as resistant, though the real problem is overload. A younger adult with a learning disability signs a form because everyone around them seems ready to move on. No one checks what has actually been understood.
A fair counter point is that some communication problems cannot be removed fully, especially where illness is severe or cognition changes from hour to hour. That is true. Yet this does not reduce the value of adapting the environment, language, and pace. It increases it.
“When staff change the way they communicate, people often change the way they respond.”
How barriers can be reduced through better practice and person centred care
Barriers cannot always be removed, but many can be reduced. The starting point is person centred communication. Staff need to think about hearing, sight, memory, literacy, language, anxiety, culture, autism, fatigue, and pain before the conversation begins. A quieter space, better lighting, eye level positioning, and a slower pace can improve an interaction straight away. The NHS guidance on communicating with people with hearing loss gives practical examples such as facing the person, reducing background noise, and speaking clearly rather than shouting.
It also helps to make information easier to process. Staff may use shorter sentences, one idea at a time, visual prompts, easy read formats, or a written summary after the conversation. They should check what the person has taken from the discussion rather than only asking, ‘Do you understand?’ For people living with dementia, tone, facial expression, and reassurance can carry as much weight as words. For people with aphasia, extra time and simple choices may support expression without taking over. For autistic people, sensory load, predictability, and direct language may shape whether communication feels manageable at all.
Consistency is another part of good care. When staff learn what works, that information should be recorded and shared. Communication passports, care plans, handovers, and input from family or unpaid carers can all help. Yet family input should support the person’s voice, not replace it. The Accessible Information Standard is especially relevant here because it focuses on identifying and meeting information and communication needs across services.
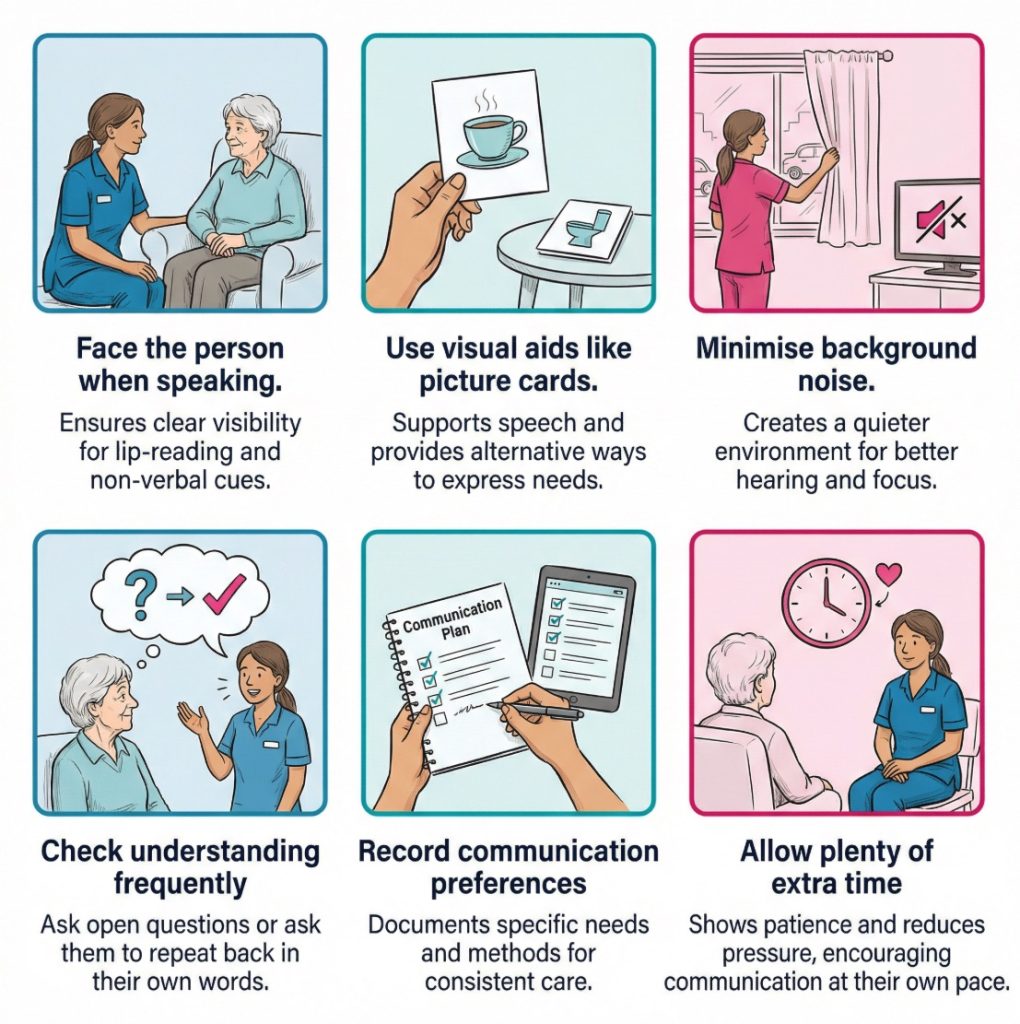
A practical checklist can help services stay focused:
- Identify the need: Notice sensory loss, cognitive change, literacy issues, language barriers, and emotional distress early. Small clues often appear before a major communication breakdown.
- Record what works: Write down useful details such as preferred pace, visual aids, quiet environments, best times of day, and whether the person lip reads or uses symbols.
- Reduce avoidable noise: Turn off televisions, move away from busy corridors, and avoid speaking while walking away or looking at a screen.
- Use accessible formats: Large print, easy read, picture prompts, hearing support, interpreters, and communication tools may widen access.
- Check the message: Ask the person to tell you what they have heard or what will happen next. This tests clarity more honestly than a quick yes or no.
- Share across the team: Good communication support should not depend on one experienced worker being on shift.
- Review regularly: Needs can change with illness, tiredness, medication, stress, or progression of a condition.
Common mistakes are worth naming because they are so familiar:
- Using jargon: Technical language can sound efficient to staff but confusing to the person receiving care. Plain English is usually safer.
- Rushing silence: Some people need longer to process and reply. Filling every pause can shut communication down.
- Assuming agreement: A nod may mean politeness, not clear consent or real understanding.
- Talking over the person: Family members and colleagues may add useful context, but the person should not disappear from the exchange.
- Treating behaviour as the whole story: Agitation, withdrawal, or refusal may be signs that the communication method has failed.
Conclusion and next step
Barriers to communication in health and adult social care include far more than speech problems or language differences. Hearing loss, sight loss, dementia, stroke, learning disability, autism, low literacy, anxiety, pain, noise, poor routines, and rushed systems can all get in the way. Often these barriers overlap. A person may be tired, hard of hearing, frightened, and surrounded by unfamiliar staff at the same time.
Poor communication can lead to confusion, distress, loss of dignity, missed symptoms, weaker consent, and support that feels impersonal. For staff, it can lead to repeated work, avoidable mistakes, and strained relationships. Clear communication will not fix every difficulty in care. It can, however, reduce risk, protect choice, and help people feel seen and heard.
The next step is usually simple. Look at the interaction, not just the individual. Ask what in the setting, timing, language, or routine might be blocking the message. Then adapt. That shift can change the whole quality of care.
“Communication is not separate from care. It is one of the ways care is delivered.”
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.
Free Communication Skills Training Course
Start a free course with Care Learning today. Certified training with interactive elements, videos and mobile friendly.





