
Positive risk taking is a person-centred approach that supports someone to do things that are important to them, even when there is some risk, by weighing the possible benefits and harms and putting sensible support in place.
Positive risk taking does not mean being careless. It does not mean ignoring danger, stepping back too far, or leaving people without support. It means looking at real life as it is. Most daily activities carry some risk. Walking outside, making a drink, seeing friends, travelling alone, handling money, starting work, or choosing what to eat all involve some uncertainty.
In health and social care, the idea is simple. A person should not lose ordinary freedoms just because support staff are worried about what might go wrong. Staff still have a duty of care. They still need to assess risk, plan support, and respond to warning signs. They also need to respect the person’s wishes, abilities, and right to make choices about their own life.
This sits closely with person-centred care, shared decision making, and least restrictive practice. It also links to the legal framework around care and support. The Mental Capacity Act 2005 says a person should be assumed to have capacity unless shown otherwise, and it says someone is not to be treated as unable to make a decision just because they make an unwise one. The Care Act 2014 places wellbeing at the centre of adult care and support. The Care Quality Commission expects services to work with people to manage risks in a way that is safe and supportive.
“Good care does not remove every risk from life. It helps a person live with choice, dignity, and support.”
Positive risk taking is not a side issue. It runs through everyday care. It affects how staff support independence, privacy, recovery, relationships, routines, and self-respect. It also shapes how services record decisions, review care plans, and explain why a person is being supported to do something rather than being stopped from doing it.
Why is positive risk taking important?
People do not build confidence by having every choice taken away. They do not keep skills by never using them. They do not feel respected when every decision is made for them in the name of safety. Positive risk taking is important because care should support a full life, not just a tightly controlled one.
For some people, the loss caused by overprotection can be serious. A person who is never allowed to make a hot drink may lose kitchen skills. A person who is stopped from going out alone may become more isolated. A person who is never trusted with their own routine may feel powerless. Over time, those losses can affect confidence, mood, identity, and independence.
Still, safety remains part of good care. Staff cannot ignore abuse, neglect, self-neglect, serious falls risk, exploitation, or acute distress. The point is not to choose freedom over safety as if one cancels out the other. The point is to look for the safest workable option that still leaves room for ordinary life. That approach reflects the broad direction of NICE guidance on shared decision making, the Skills for Care resource on working with risk, and SCIE material on person-centred care.
A common counterpoint is that a stricter approach keeps people safer. Sometimes it does, at least in the short term. A person who is stopped from walking to the local shop alone is less likely to fall on that journey. Yet a blanket ban can create different harms. The person may become less active, less confident, and more dependent. Their world may shrink. So the better question is often this: can the activity go ahead with support, review, and clear boundaries?
For staff, positive risk taking can reduce defensive practice. Defensive practice happens when the safest-looking option is chosen mainly to avoid blame. That can lead to blanket rules, excessive restrictions, and one-size-fits-all decisions. Good care is more thoughtful than that.
“A safe service is not one that says no to everything. It is one that thinks carefully before it says yes or no.”
Positive risk taking also supports trust. When people feel heard, they are often more willing to talk honestly about worries, goals, and support needs. That gives staff a stronger basis for planning care.
What laws, standards, and bodies are relevant?
Positive risk taking sits inside a clear framework of law, regulation, and professional expectation. It is not just a useful idea. It is tied to the way care should be planned and delivered.
The Mental Capacity Act 2005 is central. It sets out core principles for decision making where capacity may be in question. Two parts are especially relevant here. First, staff should presume capacity unless there is evidence to the contrary. Second, making an unwise decision does not by itself show a lack of capacity. Capacity is decision-specific and time-specific. A person may be able to decide one thing and not another. They may also need information presented in a different way, more time, or communication support.
The Care Act 2014 is also highly relevant. It places wellbeing at the centre of adult care and support. That includes personal dignity, control over day-to-day life, participation in work or recreation, family relationships, and protection from abuse and neglect. Positive risk taking fits neatly with that approach because it supports choice while still recognising safeguarding duties.
Next, regulated services need to think about the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014, Regulation 9, which covers person-centred care. The CQC quality statement on involving people to manage risks also reflects this approach. Services are expected to work with people to understand and manage risks in a balanced and person-centred way.
Other legal frameworks can shape the discussion too. The Human Rights Act 1998 is relevant where private life, dignity, autonomy, and family life are affected. The Equality Act 2010 is relevant because disabled people should not face unfair restrictions based on assumptions or stereotypes.
Important bodies and sources include:
- CQC: The regulator looks at whether services involve people in decisions about risk and use the least restrictive approach that is safe and reasonable.
- NICE: NICE guidance on shared decision making supports clear discussion about options, benefits, harms, and individual preferences.
- Skills for Care: This body provides practical resources for adult social care, including material on working with risk and enabling choice.
- SCIE: SCIE offers practice resources on person-centred care, dignity, and the Mental Capacity Act.
- Local authorities and safeguarding boards: These bodies shape local policy, thresholds, and procedures, especially where safeguarding concerns overlap with independence and choice.
A caveat here is that positive risk taking should not be treated as a fixed formula. The legal framework is clear, but care decisions still depend on the person, the setting, the level of risk, and the support available.
How does positive risk taking work in practice?
Positive risk taking usually starts with a conversation, not a ban. Staff begin by asking what the person wants to do and why it is important to them. That keeps the person at the centre of the discussion. It also stops risk paperwork from taking over too early.
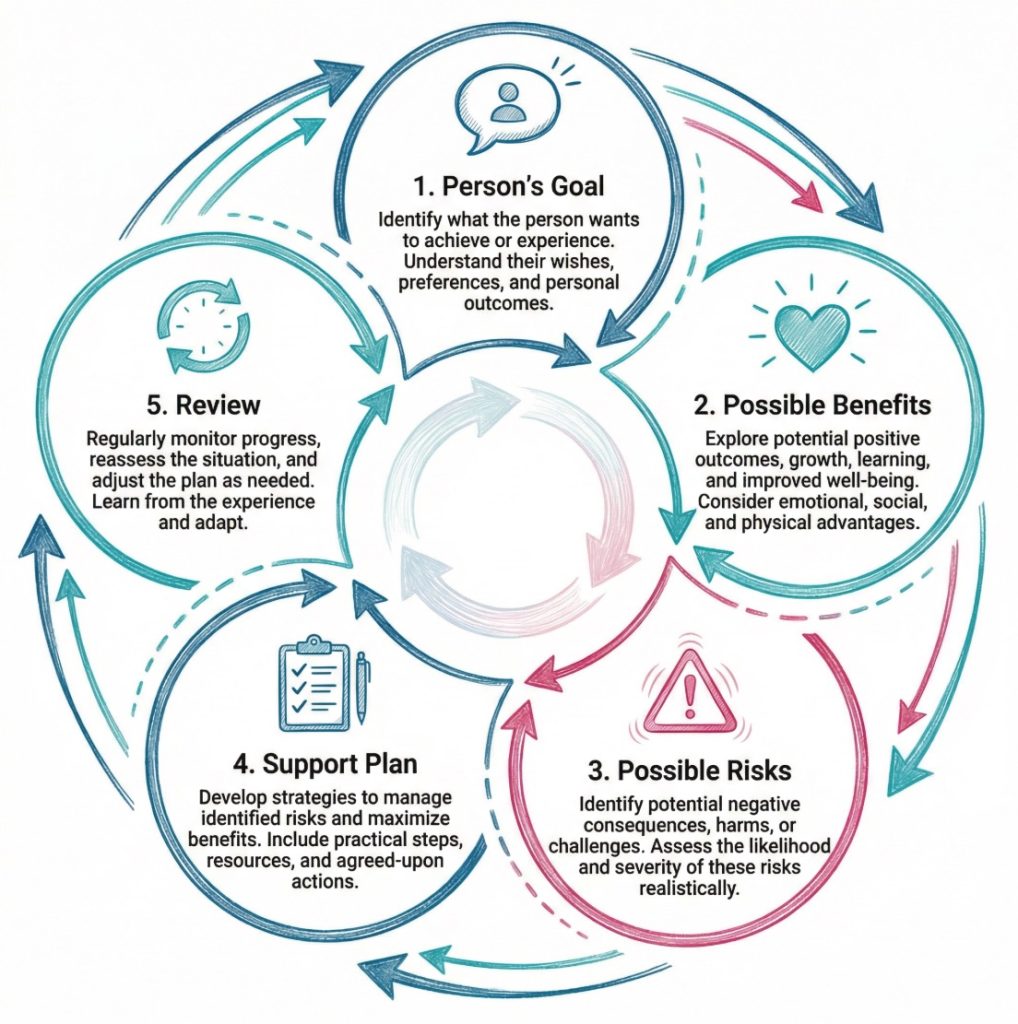
First, staff identify the goal. That goal needs to be specific. “Wants more independence” is too broad on its own. “Wants to walk to the corner shop twice a week” is clearer. Once the goal is clear, staff can look at the likely benefits. These may include confidence, routine, social contact, physical activity, privacy, recovery, or skill maintenance.
Then staff look at the risks. They need to be specific here as well. What could happen? How likely is it? How serious could it be? What signs would show that the risk is rising? This is where professional judgement comes in. A vague statement such as “at risk in the community” does not help much. A better note might say that the person becomes disorientated on unfamiliar routes after dark and may struggle to use a phone when anxious.
Meanwhile, support can be built around the activity rather than used to block it. A person who wants to cook may use adapted utensils, a perching stool, prompts, or support at busy times of day. A person who wants to travel alone may need route practice, visual prompts, a phone check-in, or a simple plan for what to do if something changes.
On second thought, it is not quite enough to say support should be “in place”. The support should also be proportionate. Too little support can be unsafe. Too much can be restrictive. That balance is where good care shows itself.
A positive risk taking process often includes:
- Clarify the goal: The person says what they want to do and why it has value for them.
- Identify the benefits: Staff look at what the person may gain, such as confidence, routine, recovery, or independence.
- Describe the risks clearly: The likely harms are set out in plain terms, not hidden behind vague language.
- Check capacity and communication needs: The person is supported to understand the decision as fully as possible.
- Plan support: Staff agree practical steps that reduce risk without taking the choice away.
- Record the reasoning: Notes explain why the activity is being supported and what safeguards are in place.
- Review the plan: The team checks what happened and adjusts the support if needed.
“The aim is not a risk-free life. The aim is a life with choice and support.”
That is how positive risk taking becomes real in day-to-day care.
When should staff use positive risk taking?
Staff should use positive risk taking whenever a person wants to do something that carries some risk but could also bring clear benefit. That covers a large part of social care and health support. Many ordinary activities fall into this area.
For example, it may come up when a person wants to cook, bathe more independently, go out alone, manage some money, start a relationship, return to work, or make decisions about their routine. It can also arise when someone chooses food or drink that is not ideal for their health, or when they want privacy in a way that makes staff uneasy. These are common situations, not rare ones.
Positive risk taking is especially relevant during change. That may be after a fall, during discharge planning, when a person moves into supported living or a care home, after a safeguarding concern, or when a condition changes. It can also be very relevant in mental health recovery, learning disability services, dementia care, reablement, rehabilitation, and home care.
Sometimes staff need to pause and tighten support first. If there is a strong and immediate risk of serious harm, abuse, neglect, exploitation, or acute illness, urgent protective action may be needed. Positive risk taking does not replace safeguarding. It sits alongside safeguarding. The CQC safeguarding framework still expects services to protect people from abuse, avoidable harm, and neglect.
Yet a pause is not the same as a permanent no. Once the immediate issue has been addressed, staff may still need to revisit the person’s original goal. That prevents short-term caution from turning into long-term restriction by habit.
Where capacity is part of the picture, timing is important. A person may be able to make one decision but not another. They may also be clearer at one point in the day than later on. Staff should support decision making before they conclude that the person cannot make the decision themselves. The Mental Capacity Act is very clear on that point.
How might positive risk taking apply in different settings?
Positive risk taking looks slightly different in each setting, though the core approach stays the same. The setting shapes the support. The person’s goal still comes first.
In home care, a person may want to keep making breakfast even though they have arthritis and reduced balance. Staff may worry about dropping pans or spilling hot drinks. A positive risk taking approach could include lighter equipment, easy-grip tools, ingredients laid out in advance, and support nearby for the more difficult parts of the task. The person keeps the routine. Staff reduce the risk without taking over the whole activity.
In a care home, a resident may want to walk to the local shop on their own. The risks may include falls, confusion, or getting delayed. A balanced response could involve checking the route, agreeing the best time of day, making sure the person has suitable shoes, carrying a phone or card with contact details, and reviewing how the first few trips go. The outing stays possible.
In supported living, a person with a learning disability may want to travel independently to college or work. Staff may help with travel training, visual prompts, emergency contacts, and practice runs before the person goes alone. Over time, the support can reduce if confidence grows.
In mental health services, a person may want to return to volunteering after a period of severe anxiety or depression. Staff may worry that the pressure will be too much. A gradual plan may work better than an outright refusal. One short session each week, clear coping strategies, and planned review points can support progress while still keeping an eye on signs of distress.
Hospital discharge can raise similar issues. A patient may want to return home rather than move into more restrictive care. The team may need to consider mobility, medication, support from family, equipment, and follow-up visits. Positive risk taking here is often about avoiding unnecessary restriction while still being honest about the support needed.
Examples across settings include:
- Daily living: A person continues to shower with equipment and checks rather than having staff do the whole task.
- Community access: A person attends a local activity with a travel plan and agreed contact points.
- Relationships: A person is supported to make choices about friendships or intimacy while staff remain alert to coercion or abuse.
- Work and study: A person returns gradually to college, training, or volunteering with review points built in.
- Health decisions: A person is involved in treatment choices through clear discussion of options, likely benefits, and possible side effects.
These examples show the same pattern. Staff do not ignore risk. They also do not assume risk is a reason to remove the activity.
How should staff assess, plan, and review positive risks?
Assessment, planning, and review turn positive risk taking from a good intention into workable care. Without them, staff may act on worry, routine, or personal opinion. With them, the decision is easier to explain and more consistent across a team.
A good assessment starts with the person’s goal. It should explain what the person wants to do and why they want to do it. That may sound obvious, but it is often missed. Risk paperwork can become so focused on harm that it barely mentions the value of the activity itself. When that happens, the decision is already skewed.
Next, the assessment should set out the likely benefits and the likely harms in plain language. Staff should also record the person’s strengths. That may include insight, physical ability, routines, communication skills, willingness to ask for help, previous success, or support from family and friends. A balanced assessment does not describe the person only through deficits.
The plan then needs to be specific. It should say what support is agreed, who will provide it, what warning signs to look for, and when the plan will be reviewed. Vague wording creates confusion. Clear wording gives staff something they can actually follow.
A useful plan often covers:
- The goal: What the person wants to do.
- The support: Equipment, prompts, supervision, timing, or communication aids.
- Named roles: Which staff, professionals, or relatives are involved and what each one will do.
- Warning signs: What may show the risk is increasing or the plan is not working.
- Review points: When the team will revisit the plan and what they will look at.
Review is just as important as the first assessment. A plan that was right three months ago may now be too restrictive or too loose. A person may gain confidence, build skills, or recover strength. Equally, new risks may appear. Regular review prevents care plans from becoming stale.
For what it is worth, some of the strongest practice is quite simple. Staff know the person well, write clearly, and keep talking to each other. Good records help, but thoughtful care starts with observation and honest discussion.
A short checklist can help teams stay focused:
- Person’s view recorded: The notes show what the person wants and why.
- Benefits listed: The plan explains what the person may gain from the activity.
- Risks described properly: The likely harms are specific and realistic.
- Support is proportionate: The response fits the risk and does not go further than needed.
- Capacity considered: Decision making support has been offered where relevant.
- Review date set: The plan will not sit untouched for months.
How can staff support positive risk taking step by step?
A step-by-step approach helps staff stay calm and systematic. It also makes the reasoning easier to record and explain.
First, staff start with the person’s goal. They ask what the person wants to do and what that activity means to them. Then they look at the likely benefits. This keeps the discussion grounded in the person’s life rather than in generic risk language.
Next, staff identify the specific risks. They consider what might happen, how likely it is, and how serious it could be. They also think about communication, timing, the environment, and any patterns in the person’s presentation. Some people cope well in the morning but struggle later in the day. Some manage familiar settings well but become anxious in crowded places.
After that, staff consider capacity and communication support. They check whether the person can understand, weigh, and communicate the decision, with help if needed. They should not jump from “I disagree with this choice” to “this person lacks capacity”. Those are different questions.
Then comes support planning. This is where the team looks for practical ways to reduce risk without removing the choice. Equipment, prompts, route planning, supervision, rehearsal, adapted routines, or agreed check-ins may all help. Often, a gradual start works well.
A simple step-by-step guide looks like this:
- Step 1 – define the goal: The person explains what they want to do.
- Step 2 – explore the value: Staff ask why the activity is important to them.
- Step 3 – map the risks: The team identifies what could go wrong and how serious it may be.
- Step 4 – support decision making: Information is shared clearly and capacity is considered where relevant.
- Step 5 – agree safeguards: Practical support is planned around the activity.
- Step 6 – record the decision: The notes explain the reasoning, the support, and any limits.
- Step 7 – try the plan: The activity goes ahead in the agreed way.
- Step 8 – review the outcome: Staff and the person look at what worked and what needs to change.
Different roles may contribute at different points:
- Care workers: Often know the person’s routine, preferences, and early warning signs best.
- Nurses: May spot clinical risks, medication issues, or health changes.
- Occupational therapists: Can suggest equipment, adaptation, and graded ways to build independence.
- Social workers: Often help balance wellbeing, safeguarding, rights, and family concerns.
- Managers: Support consistent decision making, recording, supervision, and review.
Sometimes the best step is a small one. Then another. That is often how confidence grows.
What are realistic examples of positive risk taking?
Realistic examples make the idea easier to picture. They also show the difference between sensible support and either overprotection or neglect.
A woman receiving domiciliary care wants to keep making her own breakfast. She has arthritis and reduced grip. Staff worry about spills and burns. A restrictive response would be to prepare everything for her. A positive risk taking response would keep her involved. She might use a kettle tipper, easy-grip utensils, pre-prepared ingredients, and a perching stool. Staff stay nearby for the parts she finds hardest. She keeps a familiar routine and a sense of control.
A man in supported living wants to visit his brother by bus. He has a learning disability and becomes anxious if the route changes. Staff do not simply say no. They practise the route with him, create a simple visual guide, save contact details in his phone, and talk through what to do if the bus is diverted. After several supported journeys, he begins to travel more independently.
A resident in a care home wants a glass of wine at a family celebration. Staff know the person takes medication that can increase drowsiness. The response is not a flat ban. The discussion covers the likely effects, the timing of medication, the setting, and the support available on the day. The person remains part of the decision.
A person recovering from depression wants to return to volunteering. Staff worry that stress may affect their mood. The person and staff agree to begin with one short session each week, build in check-ins, and review how it feels after a fortnight. The plan supports recovery without pretending there is no risk of setback.
These examples share several features:
- Clear purpose: The activity means something to the person.
- Realistic planning: The support matches the actual risk.
- Shared discussion: The person is involved, not spoken about from a distance.
- Proportionate support: Staff do not take over more than they need to.
- Review built in: The first plan is not treated as the final word.
“Positive risk taking is often quite ordinary. It shows up in cups of tea, bus journeys, family visits, and daily routines.”
That is one reason the topic deserves careful attention. It affects ordinary life every day.
What are common mistakes in positive risk taking?
Common mistakes usually happen when services drift too far in one direction. They become overprotective, or they become underplanned. Positive risk taking works best in the middle.
One mistake is treating safety as the only goal. A service may look safe on paper because staff stop people from doing many things. Yet the person may become bored, dependent, isolated, or frustrated. Restriction can be harmful when it goes further than the real risk justifies.
Another mistake is assuming that disagreement means lack of capacity. A person may choose something a relative or worker would not choose. That does not, on its own, mean they lack capacity. The law is clear on that point. Staff need to assess capacity properly, and only when the decision requires it.
Poor recording is another problem. If the plan is not written down clearly, staff may respond differently from shift to shift. One worker may support the activity. Another may stop it because they do not know the reasoning behind the plan. Inconsistent care can unsettle the person and increase tension within the team.
Other common mistakes include:
- Blanket rules: A service applies one rule to everyone rather than looking at individual ability and circumstance.
- Missing the person’s voice: Decisions are driven by staff anxiety or family pressure instead of the person’s own goals.
- Ignoring strengths: The assessment lists only what could go wrong and says little about what the person can do.
- No review: The plan stays in place long after the person’s abilities or needs have changed.
- Too much jargon: Terms such as capacity, least restrictive, or proportionate are used without clear explanation.
A short comparison can help here:
- Overprotective approach: Stops the activity because there is some risk.
- Reckless approach: Allows the activity with little thought or support.
- Positive risk taking: Supports the activity with planning, discussion, safeguards, and review.
That middle option is usually the one services should aim for.
What should readers take away from positive risk taking?
Positive risk taking is about supporting people to live real lives. It accepts that risk is part of daily life and that too much restriction can do harm of its own. Good care does not ignore risk. It also does not treat risk as a reason to remove choice at the first sign of uncertainty.
The strongest approach is person-centred, planned, and specific. Staff start with the person’s goal, look honestly at the risks and benefits, support decision making, agree practical safeguards, and review the plan over time. That approach fits with the Mental Capacity Act 2005, the Care Act 2014, and current CQC expectations.
The practical takeaway is straightforward. Good support asks, “How can this be done as safely as possible?” rather than “How can this be stopped?” That shift in thinking can change everyday care in a very concrete way.
A final checklist brings the topic together:
- Start with the person: Their goal should shape the discussion.
- Name the benefits: Independence, confidence, recovery, and routine should be recorded clearly.
- Be specific about risk: Avoid vague wording and generic fears.
- Support decision making: Give information in a way the person can use.
- Use the least restrictive option: Keep support proportionate to the actual risk.
- Record the reasoning: Clear notes support consistency across the team.
- Review regularly: Plans should change when the person’s situation changes.
Positive risk taking is not about taking chances with people. It is about taking people seriously.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.





