
CQC registration is the process of applying to the Care Quality Commission for registration to carry on one or more regulated health or adult social care activities in England. In plain terms, it is how a provider shows that it is legally allowed, prepared and suitable to run a regulated care or health service.
CQC does not only register a business name. It registers the legal provider, the regulated activities, the location or locations, and, where required, the registered manager. A regulated activity is a type of care or treatment covered by CQC registration rules.
Examples include personal care, accommodation for people who need nursing or personal care, nursing care, and treatment of disease, disorder or injury. CQC explains these areas in its scope of registration guidance.
A good application shows more than a business idea. It shows that the service is safe, realistic and ready to protect people from avoidable harm. CQC will look at leadership, staffing, training, finances, policies, procedures, governance systems and how people using the service will be supported.
A home care agency that helps people with washing, dressing, continence care, oral care or medicines support linked to personal care will usually need to consider registration for personal care. CQC gives more detail in its personal care regulated activity guidance.
CQC wants to see whether the provider understands the service, the people it will support, the risks involved and the systems needed to manage those risks.
Useful starting points include the CQC application process guidance, the CQC supporting documents guidance, the CQC statement of purpose guidance and the CQC register as a provider guidance.
Why CQC Registration Is Important Before Starting a Service
CQC registration helps protect people who may rely on care or treatment at vulnerable points in their lives. Before registration is granted, CQC looks for evidence that the proposed service is likely to be safe, effective, caring, responsive and well-led.
People using regulated services may need help with intimate personal care, medicines, mobility, communication, nutrition, mental health, nursing needs or long-term health conditions. A weak service can affect people quickly, so the provider needs sound systems before care begins.
Staff benefit from that preparation too. A well-prepared provider should have clear policies, safe systems, training, supervision and escalation routes. Staff are more likely to know what to do if a person falls, refuses care, discloses abuse, misses medication, becomes unwell or raises a complaint.
CQC registration sits within a wider legal and regulatory framework. The most relevant legislation and regulations include:
- Health and Social Care Act 2008: The main legal framework for CQC regulation of health and adult social care services in England.
- Health and Social Care Act 2008 (Regulated Activities) Regulations 2014: These regulations include requirements linked to the fundamental standards for registered providers and registered managers.
- Care Quality Commission (Registration) Regulations 2009: These cover registration requirements, statement of purpose duties and notification requirements.
- Mental Capacity Act 2005: This applies in England and Wales when a person may be unable to make a specific decision for themselves. More information is available from the GOV.UK Mental Capacity Act guidance.
- Care Act 2014: This is relevant to adult safeguarding and local authority duties around care and support in England. The SCIE safeguarding adults guidance gives useful background.
- Equality Act 2010: This is relevant to protection from discrimination in workplaces and wider society, including services and public functions. The GOV.UK Equality Act 2010 guidance explains the wider framework.
- Data Protection Act 2018 and UK GDPR: These apply to how providers collect, store, share and protect personal information.
A home care provider should know how it will monitor missed visits, respond to late calls, manage staff sickness and protect lone workers. A care home provider needs clear arrangements for admission assessments, staffing, medicines, maintenance and emergencies.
A clinic will have a different risk profile. It may need systems for clinical records, consent, infection control, equipment checks and clinical governance. These are part of safe service design, not extras.
What You Should Decide Before Applying to CQC
Before starting the application, the provider should be clear about the type of service it wants to run. If the service model is unclear, the application will usually become unclear too.
The provider should decide who the service is for, what needs it will support, which regulated activities apply, where the service will operate and who will manage it. Broad phrases such as “we support everyone” or “we provide all types of care” do not tell CQC what will actually happen.
For example, a new home care agency may choose to support adults over 65 with personal care in their own homes within a defined local area, such as 5 miles (8 km) from its office. The exact area is a business and safety decision, but the provider should be able to show that travel time, staffing and management oversight are realistic.
Before applying, the provider should decide:
- Service type: Home care, supported living, a care home, a clinic or another service type should be stated clearly.
- People supported: The application should describe the age group, needs, conditions or support areas the service will cover.
- Regulated activities: These should match the actual care or treatment that will be provided.
- Operating area: The application should include the office, location, care home, clinic or geographical area.
- Management roles: The nominated individual and registered manager should be identified where required.
- Staffing arrangements: Recruitment, induction, training, rotas and cover all need to be thought through.
- Risk controls: The provider should explain assessment, care planning, audits, incidents and safeguarding.
A clear service model gives the statement of purpose, business plan, training plan and policies the same direction.
This stage helps avoid a common error: shaping the application around generic policies rather than the actual service. A strong application starts with the service itself, then uses documents to show how that service will run safely.
Simple, but often missed.
How to Choose the Right Company Structure and Setup
The company structure should be decided before the CQC application is submitted. Common provider structures include a limited company, sole trader, partnership, charity or other organisation. Many providers use a limited company because it creates a clear legal identity and makes ownership, directors, governance and responsibility easier to record.
The legal provider name should be used consistently. For an organisation, this should be the legal name registered at Companies House, with the Charity Commission or shown in relevant legal documents. If the provider uses a trading name, this should be stated clearly so there is no confusion about who the legal provider is.
The registered office address used for CQC registration should be in England and should not be a PO Box where CQC needs an address for formal service of documents. CQC’s applying as a new provider guidance explains these points in more detail.
The main roles in the application are:
- Provider: The legal person or organisation responsible for carrying on the regulated activity.
- Nominated individual: The person who represents an organisation and has responsibility for supervising the regulated activity.
- Registered manager: The person responsible for the day-to-day management of the regulated activity.
- Director or partner: A person with legal or governance responsibility within the provider organisation.
In a small new service, one person may hold more than one role. The company director may also be the nominated individual and proposed registered manager, for example. This can work, but the application should explain how that person will manage each responsibility safely.
The setup should cover practical arrangements as well as formal roles. The provider should have an office or operating base, secure records system, insurance, staff recruitment plan, training plan, business continuity plan and governance system.
A supported living provider may have a registered office, an operational office and staff supporting people in their own tenancies. The application should explain where the regulated activity is managed from and where personal care is delivered.
| Area to decide | Why it is important | Example |
|---|---|---|
| Legal provider | CQC registers the legal person or organisation | ABC Care Ltd applies as the provider |
| Trading name | This avoids confusion between legal and public names | ABC Care Ltd trading as ABC Home Care |
| Registered manager | CQC needs to know who will run the service day to day | The care manager applies as registered manager |
| Operating base | CQC needs to know where records and management are based | A secure office with locked storage and care software |
| Regulated activities | Registration must match the service provided | Personal care for a home care agency |
What Documents CQC May Need to Accept Your Application
CQC expects new provider applicants to send the correct supporting documents with their application. Its supporting documents guidance explains which documents are needed and how they help CQC assess the application.
CQC separates documents into those every new provider applicant must send and extra documents that depend on the service type. All provider applicants must send the core documents listed by CQC. A financial viability statement is also required unless the applicant is a corporate provider, NHS trust, care home, home care agency or supported living service.
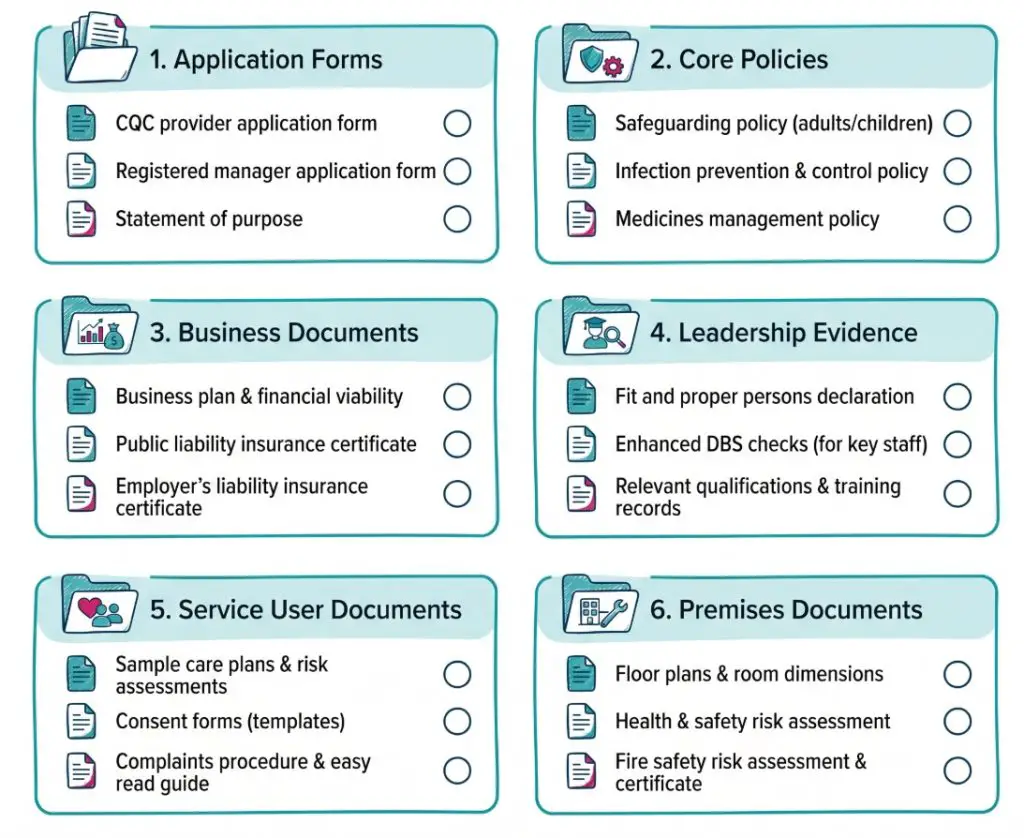
Core documents commonly include:
- Provider application form: This gives CQC information about the legal provider, regulated activities, locations and people involved.
- Registered manager application: This is needed where a registered manager is required.
- Statement of purpose: This explains what the service does, where it does it and who it supports.
- Complaints policy: This sets out how complaints will be received, investigated, responded to and used for learning.
- Consent policy and procedure: This explains how people will be involved in decisions and how consent will be recorded.
- Equality, diversity and human rights policy: This explains how people’s rights, identity, beliefs, communication needs and choices will be respected.
- Governance and quality assurance policies: These cover audits, monitoring, action plans and improvement.
- Infection prevention and control policy: This explains hygiene, PPE, cleaning, waste and infection risk controls.
- Medicines management and prescribing policy: This explains how medicines support, prescribing or transport of medicines will be managed where relevant to the service.
- Public liability and employer’s liability insurance: This shows that suitable insurance has been arranged or quoted.
- Recruitment policy: This explains safe recruitment, DBS checks, references, identity checks and right to work checks.
- Safeguarding policy and procedure: This explains how abuse, neglect and exploitation will be recognised, reported and managed.
- Financial viability statement where required: This gives CQC information about whether the provider has the financial resources to run the service safely.
Some documents are listed by CQC as extra documents for specific service types. For home care agencies, supported living services and care homes, this may include a business plan and financial forecast, service user guides and a staff training plan.
Care homes also have extra premises-related documents. These may include fire risk assessment, floor plan, gas and electrical safety certificates, legionella risk assessment, planning permissions, environmental risk assessment and evidence of legal occupancy.
CQC lists service-specific requirements in its extra supporting documents guidance. Providers applying for more than one type of service may need to send documents for each service type.
Documents should prove readiness, not fill a folder. Each document should show how the service will run safely.
Each document should include the provider name, date, review date, version number and person responsible. Draft documents, old versions and policies with another provider’s name can weaken an application quickly.
How Each Stage of the CQC Application Works
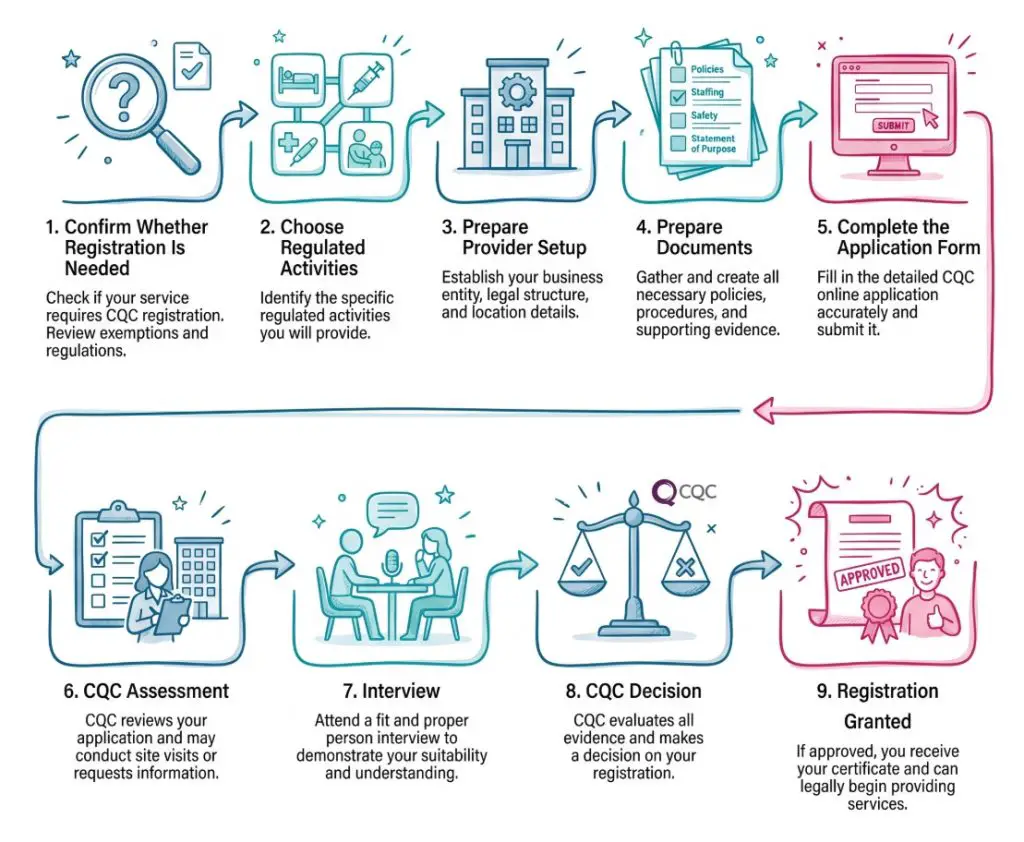
The CQC application process usually has several stages. Knowing the stages helps the provider prepare properly and avoid rushed submissions.
The first stage is confirming whether registration is needed. This means reviewing the service against CQC’s what is registration guidance. The name of the service does not decide whether registration is needed. The actual activity does.
The second stage is choosing the correct regulated activities. This should be based on what the service will actually provide. Personal care is different from general support. A service that only provides shopping, cleaning or companionship may not be carrying on the same regulated activity as a service that helps with washing, dressing or continence care.
The third stage is preparing the provider setup. This includes the legal provider, company structure, nominated individual, registered manager, office base, insurance, staffing plan and governance arrangements.
The fourth stage is preparing documents. This is where the statement of purpose, business plan, training plan, financial forecast, service user agreement or guide and policies are created. The documents should be complete and consistent.
The fifth stage is completing the application form. CQC’s provider application forms page explains how provider application forms, registered manager applications and supporting documents fit together.
The sixth stage is CQC’s assessment. CQC may review provider fitness, registered manager fitness, financial viability, governance, policies, service model and whether the proposed service is likely to meet regulatory requirements.
If the application passes CQC’s initial checks, CQC may arrange an interview, involve the nominated individual and proposed registered manager where needed, and book a site visit if one is needed.
The final stage is CQC’s decision. CQC may grant registration, grant it with conditions, ask for more information or refuse the application. A provider should not start carrying on a regulated activity until CQC registration has been granted for that activity.
Step-by-Step Guide: How to Prepare a CQC Registration Application
A step-by-step approach makes the process easier to manage. It also reduces the risk of inconsistent documents or missing evidence.
- Step 1: Check whether the service needs CQC registration: The provider should look at the actual care, support or treatment it will provide. A “support service” may still need registration if it provides personal care.
- Step 2: Identify the regulated activities: The service should be matched to the correct regulated activities. Home care agencies often consider personal care. Some clinics may need treatment of disease, disorder or injury.
- Step 3: Decide the legal provider structure: The provider may be a limited company, sole trader, partnership, charity or other organisation. The legal name should stay consistent across all documents.
- Step 4: Appoint responsible people: The nominated individual and proposed registered manager should be identified where required. They should know their duties and be able to explain them clearly.
- Step 5: Build the service model: The provider should describe who the service is for, what it will provide, what it will not provide, where it will operate and how it will be staffed.
- Step 6: Prepare the business plan and forecast: The plan should show that the service is financially realistic. It should include wages, training, insurance, rent, software, equipment, travel time and contingency.
- Step 7: Prepare the statement of purpose: The statement of purpose should accurately describe the service, regulated activities, locations, provider details and management arrangements.
- Step 8: Prepare policies and procedures: Policies should match the service. Documents that mention another provider, another service type or irrelevant procedures should not be used.
- Step 9: Prepare the training plan: The plan should show how staff will be inducted, trained, supervised and assessed as competent. Skills for Care’s Care Certificate standards can help providers think about induction for new care workers.
- Step 10: Prepare the service user agreement or guide: This document should explain what people can expect from the service, including care planning, rights, complaints, confidentiality and fees where relevant.
- Step 11: Check every document for consistency: Names, addresses, regulated activities, roles, locations and service descriptions should match across all documents.
- Step 12: Complete and submit the application: The provider should use the current CQC route for the service type. CQC says the application must be completed by the provider, and manager forms must be sent with the provider application where they are needed. All required documents should be submitted together.
- Step 13: Prepare for the CQC interview: The responsible people should practise explaining safeguarding, staffing, training, medicines, governance, complaints, mental capacity and quality monitoring.
This process gives the application a clear route from service idea to submission. It also helps show CQC that the provider has planned the service in a safe and organised way.
How to Fill in the Online CQC Application Form and Use the CQC Portal
Some providers may be able to use an online registration route, especially where CQC signposts this for personal care services. Other new provider applications may use downloadable forms and email submission. The route depends on the service type and the current CQC process, so the provider should use the current CQC registration pages rather than relying on older saved forms.
Every answer in the application should be treated as evidence. Broad statements such as “we will provide good care” or “we will follow all guidance” do not explain how the service will run.
A stronger answer explains the system. Instead of writing “we will monitor quality”, the provider could explain that the registered manager will complete monthly audits of care plans, medicines records, complaints, incidents, safeguarding concerns, staff files and training records.
The answer could then explain that findings will be added to an action plan and reviewed at management meetings. That gives CQC a clearer picture of how the provider will check safety and quality.
Good answers usually explain:
- What will happen: The process should be described clearly.
- Who is responsible: The role should be named, such as registered manager, care coordinator or senior care worker.
- When it will happen: The answer should give a clear frequency, such as before care starts, monthly or after an incident.
- How it will be recorded: The answer should explain the record, form, care software or audit tool.
- How improvement will happen: The answer should show how learning will lead to action.
The application form should match the supporting documents. If the form says the service will support people living with dementia, the training plan should include dementia training. If the statement of purpose says the service will provide medicines support, the medicines policy should explain how staff will support medicines safely.
Use clear file names when uploading or sending documents. For example:
- Statement of Purpose: Statement of Purpose, ABC Care Ltd, April 2026.
- Safeguarding Policy: Safeguarding Policy, ABC Care Ltd, April 2026.
- Training Plan: Training Plan, ABC Care Ltd, April 2026.
- Business Plan and Financial Forecast: Business Plan and Financial Forecast, ABC Care Ltd, April 2026.
Draft documents, old versions and policies with another provider’s name can suggest poor governance. Small errors can raise bigger doubts.
What to Include in a CQC Business Plan
A CQC business plan should show that the service is realistic, sustainable and safe. It should not read like a sales brochure. It should explain how the provider will operate safely, manage growth and maintain enough resources.
For a home care agency, the plan may include the geographical area, personal care tasks, visit planning, staff rotas, travel time, out-of-hours arrangements, referral sources and how packages will be accepted safely.
A care home plan may look different. It may cover the number of beds, occupancy assumptions, staffing model, dependency levels, premises arrangements, admission process and emergency planning.
A strong business plan may include:
- Provider overview: The legal provider, ownership, leadership and purpose.
- Service description: What the service will provide and who it will support.
- Regulated activities: A clear link between the service and the regulated activities being applied for.
- Market and referrals: Where referrals may come from, such as private clients, local authorities, NHS routes or direct enquiries.
- Staffing plan: Roles, recruitment, rotas, induction, supervision and cover.
- Financial forecast: Wages, travel, insurance, training, rent, software, equipment and contingency.
- Risk management: How care, staffing, financial and operational risks will be monitored.
- Quality assurance: Audits, complaints, incidents, feedback and improvement plans.
- Growth plan: How the service will grow at a safe pace.
A realistic new home care agency might start with five to ten care packages, then grow once recruitment, supervision and quality checks are stable. A weaker plan would claim the agency can support one hundred people straight away without showing how staff will be recruited, trained and managed.
The financial plan should connect directly to safety. If travel time, holiday pay, training time, management time and sickness cover are not included, the service may struggle to operate safely. Financial pressure can lead to rushed visits, missed calls, poor supervision and weak recruitment.
A business plan should show how safe care will be funded, staffed and monitored. It should not only describe growth.
Restraint can strengthen the plan. Some new providers want to take every referral quickly, but safer growth means accepting work that matches staff skills, management capacity and the provider’s registration.
What to Include in a CQC Training Plan
A training plan should show how staff will become competent and how competence will be maintained. A training certificate alone does not prove that a staff member can carry out a task safely. Competence means the person can apply knowledge correctly in real situations.
A care worker may complete medicines training online. The provider should still check whether they can read a medicines administration record, follow a care plan, record support correctly and report a medicines error.
Skills for Care provides useful material on induction for health and social care workers. Providers may also use the Skills for Care induction toolkit to plan how new staff are introduced to the service.
Skills for Care’s 2025 Care Certificate standards can help providers plan induction for new health and social care workers. The standards describe knowledge, skills and behaviours for specific roles, and workers need to be assessed on what they know and what they do.
A good training plan should include:
- Induction training: Introduces the provider’s values, policies, systems and basic safety expectations.
- Mandatory training: Covers essential subjects such as safeguarding, infection control, health and safety, moving and handling, equality and record keeping.
- Role-specific training: Matches the service user group, such as dementia, autism, learning disability, diabetes awareness or end-of-life care.
- Competency checks: Shows how managers will observe practice and sign staff off for specific tasks.
- Refresher training: Sets out how often training will be updated.
- Supervision and appraisal: Shows how staff learning and performance will be reviewed.
- Training records: Tracks completed, due and overdue training.
Training should match the service. A supported living service for people with learning disabilities may need training on communication, positive behaviour support, autism awareness and mental capacity. A care home supporting older people may need training on falls, nutrition, pressure care, dementia and medicines.
A home care agency may need strong training around lone working, moving and handling in people’s homes, medicines prompts and visit recording. The training plan should not be a long list of courses with no explanation of competence.
A new care worker might complete induction, shadow experienced staff, complete required training and then be observed before working alone. A senior care worker may receive extra training in supervision, spot checks and care planning. A registered manager may need leadership, safeguarding management, quality assurance and regulatory knowledge.
A strong training plan shows CQC that staff will not be sent into care settings without preparation. It also helps people using the service receive safer, more consistent care.
What to Include in a Service User Agreement
A service user agreement explains the relationship between the provider and the person receiving care. It should be written in plain English so people can see what the service will provide and what they can expect.
The agreement should match the service type. A home care agreement may cover visit times, personal care tasks, access to the home, fees, cancellations, confidentiality, complaints and staff conduct.
A supported living agreement may cover personal care, support planning, key working and boundaries between housing and care. A care home agreement may include accommodation, care, fees, visitors, personal belongings and ending arrangements.
A useful service user agreement may include:
- Service description: What care or support will be provided.
- Assessment and care planning: How assessed needs shape the care or support provided.
- Person’s rights: Dignity, privacy, respect, choice and involvement.
- Staff responsibilities: Safe care, confidentiality, accurate records and respectful conduct.
- Person’s responsibilities: Access arrangements, sharing relevant information and treating staff respectfully.
- Fees and payment: Clear charges where the person pays for care.
- Changes and cancellations: How care visits or services can be changed.
- Complaints: How concerns can be raised and handled.
- Safeguarding: How the provider may act if someone appears at risk.
- Confidentiality and data protection: How personal information will be used and protected.
If a person receives two daily home care visits, the agreement should explain the expected visit times, what staff will do, how changes are requested and how concerns are reported. This reduces confusion for the person, relatives and staff.
The agreement should also consider communication needs. Some people may need large print, easy read, translated information or support from an advocate, family member or representative. This supports person-centred care and helps people know their rights.
A good agreement is not just a contract. It is also a clear explanation of how the service will behave, communicate and respond when plans change.
What a Statement of Purpose Should Cover
The statement of purpose is one of the most important CQC registration documents. It explains what the provider does, where it does it and who the service is for. CQC’s statement of purpose guidance explains the role of this document and why it must be kept accurate.
The statement should be clear, factual and specific. It should not read like an advert. It should not promise services that the provider is not ready or registered to provide.
A statement of purpose should usually include:
- Provider details: Legal name, trading name, address, contact details and legal status.
- Aims and objectives: The purpose of the service and how it intends to support people.
- Regulated activities: The regulated activities being applied for.
- Service user groups: Who the service is for.
- Locations: Where the service is managed from and where care is provided.
- Registered manager details: Who manages the regulated activity.
- Nominated individual details: The nominated individual where the provider is an organisation.
- Service description: What the service provides in practical terms.
- Quality and safety approach: How risks and quality will be monitored.
A clear statement might say that the provider offers personal care to adults in their own homes, including support with washing, dressing, continence care, oral care, meals linked to personal care and medicines support where included in the care plan.
That is stronger than saying “we provide excellent support to vulnerable adults”. CQC needs a clear description, not promotional wording.
The statement should match the application form, policies, business plan and service user agreement. If the statement of purpose says the service supports people with dementia, the training plan should include dementia training and the care planning policy should explain how communication, capacity and changing needs will be managed.
If the statement of purpose is revised, CQC’s registration regulation guidance says written details of the revision must be provided to CQC within 28 days. If the change affects regulated activities, locations or other registration conditions, a separate registration change may also be needed.
What Policies and Procedures Are Required for CQC Registration
Policies and procedures explain how the provider expects the service to work. A policy sets out the provider’s approach. A procedure describes the steps staff should follow.
For CQC registration, policies should be practical, current and tailored to the service. Generic policies can create problems because they may not reflect the real risks in the service. A care home policy may not fit a home care agency. A clinic policy may not fit supported living.
CQC’s documents everyone must send guidance lists core documents for new provider applications. These include complaints, consent, equality and human rights, governance and quality assurance, infection prevention and control, medicines where relevant, recruitment and safeguarding.
The following policies include CQC’s core supporting documents and other policies that may be relevant depending on the service. Some policies may not need to be submitted with the first application unless CQC asks for them, but the provider should still have systems that match the service being proposed.
Useful policies for a new care provider may include:
- Safeguarding adults policy: Abuse, neglect, reporting routes, immediate protection and record keeping.
- Complaints policy: How complaints are received, acknowledged, investigated, responded to and reviewed.
- Consent policy: How staff seek consent and what happens if capacity is unclear.
- Mental capacity policy: Decision-specific capacity and best interests processes.
- Recruitment policy: Safe hiring, references, DBS checks, identity checks and right to work checks.
- Induction and training policy: How staff are prepared before working alone.
- Supervision and appraisal policy: How staff practice is reviewed and supported.
- Medicines policy: Safe medicines support where this forms part of the service.
- Infection prevention and control policy: Hygiene, PPE, cleaning and infection risk controls.
- Health and safety policy: Risk assessments, accidents, incidents and safe working. The Health and Safety Executive health and social care guidance is a useful reference point for workplace safety duties.
- Lone working policy: How staff working alone are protected.
- Moving and handling policy: Safe support, equipment and risk assessments.
- Equality, diversity and human rights policy: Fair, respectful and rights-based care.
- Confidentiality and data protection policy: How personal information is protected.
- Whistleblowing policy: How staff can raise concerns.
- Incident and accident reporting policy: Recording, escalation, investigation and learning.
- Care planning and risk assessment policy: Assessment, planning, review and person-centred care.
- Business continuity policy: How the service will respond to disruption.
- Record keeping policy: Accurate, timely and respectful care records.
Policies should include the provider name, date, review date, version number and person responsible. They should be accessible to staff and used during induction, supervision and audits.
A stronger set of policies will show how staff act when something happens. A safeguarding policy should not only describe abuse. It should explain what a worker does when they see unexplained bruising, hear a disclosure, suspect neglect or believe a person is being financially exploited.
How Policies Should Work Day to Day
Policies should not sit in a folder untouched. CQC may ask how policies are used in everyday work. A provider should be ready to explain how staff learn about policies, how managers check knowledge and how practice is audited.
A safeguarding policy should connect to training, supervision, reporting and management review. Staff should know the signs of abuse and neglect. They should know what to do if a person says they are being harmed.
A practical safeguarding scenario may look like this:
- Concern noticed: A care worker sees unexplained bruising and the person appears anxious.
- Immediate action: The worker checks whether the person is safe and reports the concern to the manager.
- Recording: The concern is recorded clearly, using factual language.
- Escalation: The manager follows the safeguarding procedure and contacts the relevant safeguarding route where needed.
- Review: The manager considers whether other people may be at risk and whether staff need further support.
Complaints need the same practical thinking. If a family member says evening visits are often late, the manager should review call logs, rota planning, travel time and staff feedback. If the complaint is upheld, the provider explains the outcome and changes the system where needed.
A governance policy should create a routine for checking quality. This may include monthly audits of care plans, medicines records, incidents, complaints, safeguarding concerns, staff files and training records.
Medicines policies need particular care. A home care provider may need to reflect NICE guidance on medicines support for adults receiving social care at home. A care home may need to reflect NICE guidance on managing medicines in care homes.
Policies should help staff know what to do and help managers identify problems early.
How to Prepare for the CQC Interview
The CQC interview is often used to check whether the provider, nominated individual or proposed registered manager knows the service well enough to lead it safely. It is not enough to know where the policies are stored. The person being interviewed should be able to explain how the service will run.
CQC may use the interview to explore safeguarding, staffing, recruitment, training, care planning, risk assessment, medicines, mental capacity, complaints, governance, infection control and leadership. A DBS check can support safer recruitment, but it is only one part of a wider recruitment process.
A good interview answer usually includes:
- Principle: Clear knowledge of the subject.
- Process: What will happen in the service.
- Example: A realistic situation.
- Oversight: How the provider will check that the process works.
If asked about recruitment, a weak answer would be “we will do DBS checks”. A stronger answer would explain the full process: application form, interview, identity check, employment history, references, right to work check, DBS check, induction, probation and supervision. The Disclosure and Barring Service employer guidance is a useful source for checking roles and DBS request routes.
Interview preparation should include reading every submitted document. Answers should match the statement of purpose, policies, business plan and training plan.
Useful preparation activities include:
- Scenario practice: Tests judgement and safe decision making.
- Regulated activity review: Confirms what the service is applying to provide.
- Service user group review: Focuses on the needs, risks and support required.
- Governance examples: Helps the registered manager explain audits, action plans and learning.
- Realistic service limits: Keeps the application within what the service is ready to support.
- Clear risk thinking: Shows what happens when something goes wrong.
A new provider may feel that CQC asks for a great deal of evidence before any care has been delivered. The reason is straightforward: once personal care or treatment starts, weak systems can affect real people quickly. Registration checks readiness before people are placed at risk.
The interview should show that the manager is prepared, reflective and able to lead. CQC is unlikely to expect a new service to be perfect, but it will expect clear systems and safe judgement.
Mock CQC Interview Questions and Example Answers
Mock questions help applicants practise clear, practical answers. The examples below should be adapted to the actual service.
Question: How will you make sure people are safe?
Example answer: I would start with a full assessment before care begins. This would include mobility, medicines, nutrition, skin integrity, communication, mental capacity, safeguarding risks and the home environment where relevant. Care plans and risk assessments would be reviewed regularly and sooner if needs changed. I would also use staff training, supervision, spot checks, audits, incidents, complaints and feedback to monitor safety.
Question: What would you do if a care worker reported a safeguarding concern?
Example answer: I would first consider whether the person is in immediate danger. If urgent action was needed, I would act straight away. I would record the concern clearly, report it through the correct safeguarding route and follow our safeguarding procedure. I would also consider whether other people may be at risk and what learning should follow.
Question: How will you know staff are competent?
Example answer: I would not rely only on training certificates. Staff would complete induction, shadowing, observed practice and competency checks. For higher-risk tasks such as medicines support or moving and handling, staff would need specific training and observed competence before working alone.
Question: How will you manage medicines safely?
Example answer: Medicines support would be included in the assessment and care plan. Staff would only support medicines if they had been trained and assessed as competent. Records would be completed at each visit or medicine round. Any error, missed dose, refusal or concern would be recorded, escalated and reviewed.
Question: How will you manage complaints?
Example answer: I would make the complaints process easy to access and explain it when people start using the service. Complaints would be recorded, acknowledged, investigated and responded to clearly. I would look for themes, such as lateness or poor communication, and use findings to improve the service.
Question: What would you do if a person refused care?
Example answer: I would respect the person’s right to make choices where they had capacity for that decision. Staff would offer information, check understanding and avoid pressure. If refusal created risk, staff would record it and escalate it. If there were concerns about capacity, we would follow our mental capacity procedure.
Question: How will you keep the service well led?
Example answer: I would use audits, supervision, staff meetings, incident reviews, complaints reviews and action plans. I would keep records accurate and review them regularly. I would also encourage staff and people using the service to raise concerns early.
The best mock answers sound grounded. They explain what happens, who acts, what gets recorded and how the manager checks the outcome. That is what turns a policy into a working system.
Where CQC Registration Looks Different in Different Settings
The CQC registration process follows the same broad principles, but the evidence may look different depending on the setting. A home care agency, supported living service, care home and clinic will not need identical documents or risk controls.
Home care agency example:
A home care agency providing personal care should explain how visits will be planned, how staff travel time will be managed, how missed visits will be monitored and how people will be assessed before care starts. The provider should also show how lone workers will be supported and how care records will be completed in people’s homes.
Supported living example:
A supported living provider may support people in their own tenancies. If the provider delivers personal care, registration may be needed. The application should clearly separate housing from care where this applies. Policies should cover person-centred care, safeguarding, mental capacity, communication, staff boundaries and positive behaviour support where relevant.
Care home example:
A care home application will usually need more premises-related evidence. This may include fire safety, environmental risks, floor plans, safety certificates, staffing, admissions and dependency levels. The provider should explain how residents will be assessed before admission and how staffing will match people’s needs.
Healthcare clinic example:
A clinic may need to consider treatment of disease, disorder or injury. The application may need to show clinical governance, infection control, professional competence, consent, record keeping, equipment safety and emergency arrangements.
Service for autistic people or people with a learning disability:
A provider supporting autistic people or people with a learning disability should refer to CQC’s Right support, right care, right culture guidance. CQC describes this as statutory guidance for services that currently provide, or intend to provide, regulated care to autistic people and people with a learning disability.
The safest application is specific to the setting. Generic documents rarely explain the real risks people and staff will face.
These examples show why tailored documents are so important. A safe application should reflect the real setting, real risks and real needs of the people who may use the service.
Common Mistakes to Avoid in a CQC Registration Application
Many CQC registration problems come from unclear planning, inconsistent documents or generic paperwork. These mistakes can delay the application or lead to rejection.
Common mistakes include:
- Wrong regulated activity: The activities selected do not match what the service will actually do.
- Generic policies: Policies mention another provider, another service type or irrelevant procedures.
- Inconsistent names and addresses: The legal provider name, trading name, office address and location details do not match.
- Weak statement of purpose: The statement is too vague, too promotional or does not explain the real service.
- Unrealistic business plan: The forecast ignores wages, travel time, training, insurance, management costs or contingency.
- Poor training plan: The plan lists training topics but does not explain competence checks or refresher training.
- No clear governance system: The provider cannot explain how quality will be audited, reviewed or improved.
- Overpromising: The application says the service will support complex needs without showing suitable staffing, training or systems.
- Unclear registered manager role: The proposed manager cannot explain how they will manage the service day to day.
- Missing documents: Required supporting documents are not sent together or are incomplete.
- Poor version control: Documents have no dates, old review dates or different versions with conflicting information.
- Copied wording without knowledge: Interview answers do not match the submitted documents.
Another mistake is treating CQC registration as the finish line. Registration is only the starting point. Once registered, providers must continue to meet regulatory requirements, keep records, monitor quality, notify CQC of certain events and maintain safe systems.
A good application should focus on systems that will actually be used after registration. It should not be a collection of documents created only to pass the application stage.
How to Check Your Application Before Submission
A final review can prevent avoidable rejection. The aim is to make sure the application is complete, consistent and realistic.
Start with the regulated activities. The activities should match the care or treatment described in the application, statement of purpose, policies and business plan.
Then check the provider details. The legal provider name should match Companies House or the relevant legal documents. The nominated individual and registered manager should be clearly identified. The location and office base should match across documents.
A final checklist could include:
- Complete application forms: Every required section should be answered clearly.
- Supporting documents included: Required policies and service-specific documents should be attached.
- Accurate statement of purpose: It should match the service, regulated activities and locations.
- Realistic business plan: Staffing, income, costs and growth should be believable.
- Practical training plan: It should include induction, competency checks and refresher training.
- Tailored policies: They should match the provider, service type and client group.
- Insurance evidence ready: The cover should reflect the planned service.
- Premises evidence included where relevant: This is especially important for care homes, clinics and other premises-based services.
- Clear file names: CQC should be able to identify each document easily.
- Interview preparation completed: Responsible people should know the application well.
The final review should check whether the forms, statement of purpose, policies, training plan, business plan and service documents give a consistent picture of the proposed service.
Remove irrelevant material. More paperwork is not always better. Clear, accurate and service-specific documents are more useful than large files full of generic information.
Practical Takeaways for a Stronger CQC Application
A strong CQC application is built around one clear service model. The provider should know what it will provide, who it will support, where it will operate and how it will manage risk.
The documents should fit together. The statement of purpose should match the application form. The business plan should match the staffing plan. The training plan should match the service user group. The policies should match the actual service.
The following points are useful before submission:
- Be specific: Clear service descriptions are stronger than broad claims.
- Keep names consistent: The legal provider name, trading name and location details should match.
- Plan safe growth: The service should only accept work it can staff and supervise safely.
- Use tailored policies: Policies should describe how this service will operate.
- Show competent leadership: The registered manager should be able to explain the whole service.
- Connect finance to safety: The business plan should show how staffing, training and governance will be funded.
- Prepare for scenarios: CQC may ask what happens when a risk, complaint or safeguarding concern arises.
- Check every file: Missing, old or inconsistent documents can delay the application.
The strongest applications are clear and calm. They avoid exaggeration. They show steady planning, suitable knowledge and honest limits.
Good preparation shows up in small details. Matching dates. Clear file names. Policies that use the provider’s name. Interview answers that sound like the actual service, not copied text.
Conclusion and Next Step
CQC registration is a detailed process that checks whether a provider is ready to deliver regulated care or treatment safely. A strong application should be clear, consistent and practical. It should explain what the service will do, who it will support, where it will operate, who will manage it and how people will be protected.
The main documents all have a purpose. The statement of purpose explains the service. The business plan shows whether the service is realistic. The training plan shows how staff will be prepared. The service user agreement or guide explains what people can expect. Policies and procedures show how staff should work and how managers will respond when risks arise.
Good preparation also supports the CQC interview. A provider or registered manager who knows their documents should be able to explain safeguarding, complaints, medicines, staffing, training, governance and risk management with confidence.
The strongest applications avoid vague promises. They focus on real work. They show how the service will run on an ordinary day and how it will respond when something goes wrong.
Before submission, the provider should check every document carefully and only submit when the service is ready for registration assessment. CQC says applications should only be submitted when everything is in place to start providing services, including locations and staff.
A careful application gives CQC a clearer picture of readiness. It also gives the service a safer foundation from the beginning.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.