
CQC service user bands are registration categories that describe the main groups of people a service is set up to support at a registered location. They sit alongside regulated activities and the statement of purpose. They help show whether the service has the right staff, environment, policies and oversight for that client group.
A service user band is not a rating. It is not a funding band either. It is a way of describing the people a service is designed for.
The phrase sounds technical. The purpose is simple. A care home, home care agency, clinic or specialist service needs to be clear about who it supports, and that description needs to match the day to day reality.
“Service user bands describe who a service is built for, not how serious a person’s needs are.”
This sits within the wider CQC registration framework and links closely to the statement of purpose. It also connects with the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014.
What are CQC service user bands?
CQC service user bands describe the main type of people a service expects to support. They form part of the registration details for a location. A provider uses them to show the broad client group the service is designed around, such as older people, younger adults, people living with dementia or people with physical disabilities.
The word ‘band’ can throw people off. It sounds like a score or a ranking. It is neither. It is simply a category within registration, used so CQC can judge whether the service fits the people likely to use it.
That reaches beyond paperwork. Service user bands should line up with the service’s staffing model, training, care planning, admission decisions, environment and governance. A service set up for older people with dementia will usually need a different layout, pace and skill mix from a service supporting autistic adults or people with substance misuse needs.
A band should describe the main service model. It does not need to capture every condition a person may have. Many people using health and social care services have overlapping needs, and the service user band still needs to reflect the main client group the service is built around.
This is where the trainer view comes in. New staff often assume bands are just something for registration managers. They are not. They shape how a service thinks about fit, risk and daily support. Quietly, but all the time.
Several sources help fill out that wider picture. Skills for Care covers workforce planning and role development in adult social care. The Care Certificate standards set out the knowledge, skills and behaviours expected of new workers. NICE publishes guidance relevant to care quality, safety and service design. The NHS service search also shows how services are often described by the people and needs they are built around.
“A good band tells the truth about the service before a placement starts.”
Why do service user bands affect care and registration?
Service user bands affect registration because they help show whether a service is suitable for the people it supports. If the registration says one thing but the service is doing something else, the official picture stops matching reality.
Poor fit can creep in slowly. A placement may look workable on paper but still be wrong for the person. Staff may be willing. The provider may want to help. Yet the service itself may not be built for that person’s needs. The building, routines, activities, communication style and staffing may all point in another direction.
Take a care home registered for older people, dementia and physical disability. If it starts supporting a younger autistic adult whose main need is specialist behavioural support, the mismatch may be obvious. The setting may be safe in a basic sense, but it may not be suitable. The person could end up in an environment that does not reflect their age, lifestyle, communication needs or daily rhythm.
One support worker put it more bluntly: “We can do the personal care, but the whole place still feels wrong for him.” That is the point. Tasks and suitability are not the same thing.
There is also a regulatory angle. A provider must keep its statement of purpose accurate under the Care Quality Commission (Registration) Regulations 2009. The information set out in Schedule 3 includes details that explain what the service does and who it is for. If the client group changes, those details may need review.
This links to wider standards around person centred care, safe care and treatment, staffing and good governance. Those standards sit in the 2014 regulations. They also sit alongside wider duties under the Care Act 2014, the Mental Capacity Act 2005, the Mental Capacity Act Code of Practice and the Equality Act 2010. If a service takes people it is not set up for, problems can show up in consent, communication, reasonable adjustments, risk assessment and care planning.
A fair counterpoint is that many services support people with mixed needs, so rigid categories can seem too neat. That is true. Real services are rarely tidy. Still, registration has to describe the main client group clearly enough for CQC, commissioners, staff and families to see what the service is set up to do well.
“When the band and the real service drift apart, the first impact is usually on the person receiving care.”
What is the list of CQC service user bands?
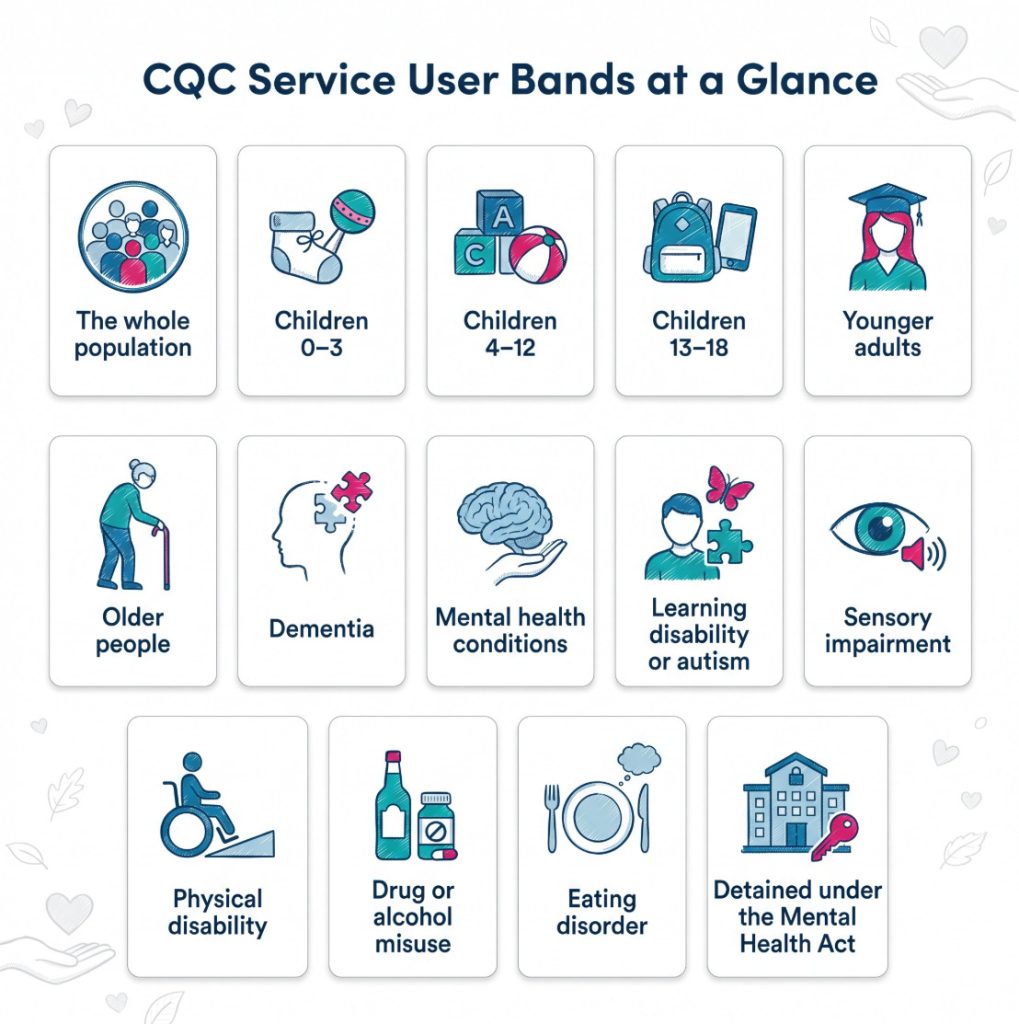
The wording can vary slightly between forms and older templates, but the commonly used CQC service user bands include the groups below. These are the broad categories providers use when describing the people a service is designed to support.
| Service user band | What it covers |
|---|---|
| The whole population | Services intended for everyone rather than a narrow client group |
| Children aged 0–3 years | Very young children with age specific safeguarding and developmental needs |
| Children aged 4–12 years | School age children whose support needs differ from toddlers and teenagers |
| Children aged 13–18 years | Older children and teenagers, often with transition and independence issues |
| Younger adults | Adults below the older people category |
| Older people | Adults in later life, often linked to frailty or age related support needs |
| People living with dementia | People whose memory, orientation or communication may be affected by dementia |
| People with mental health conditions | People whose main support need relates to mental health |
| People with a learning disability or autistic people | People needing a service model built around learning disability or autism |
| People with sensory impairment | People with sight loss, hearing loss or dual sensory loss |
| People with physical disability | People with mobility needs, neurological conditions or long term physical impairment |
| People who misuse drugs or alcohol | People whose main support need relates to substance misuse |
| People with an eating disorder | People supported in services focused on eating disorders |
| People detained under the Mental Health Act | People whose detention status forms part of the service model |
The list is broad on purpose. It is not meant to work like a detailed clinical profile. It gives a registration level picture of the service. The detail belongs elsewhere, including the statement of purpose, referral assessment and care planning.
A few examples bring that into focus.
- The whole population: A GP practice or broad community service may use this because it is open to all age groups and a wide range of needs.
- Older people: A residential care home may choose this where the whole model is built around later life support, mobility needs and long term conditions.
- People living with dementia: A service may use this when its staff training, environment and daily routines are shaped around dementia care.
- People with a learning disability or autistic people: A specialist supported living service may use this where the accommodation, staffing and support model are built around those needs.
Short list. Wide effect.
A provider should not treat the list as a way to tick every possible box. If too many bands are chosen, the description can become vague or misleading. It may suggest specialist depth that the service does not really have.
When do service user bands need to be used or reviewed?
Service user bands are usually needed when a provider registers a new service or a new location. They form part of the information CQC uses to decide whether the proposed service is suitable for the people it plans to support.
They also come into play when a provider adds a location, adds a regulated activity or changes the service model. The registration details should continue to match the actual service. If the client group changes, the statement of purpose may need updating as well.
This becomes especially important when a service broadens over time. A home care agency may start with personal care for older people, then take on support for people with dementia, and later accept packages for autistic adults or people with a learning disability. At each stage, the provider needs to consider whether the registered scope of the service still fits.
The same point applies in residential settings. A care home might begin as a service for older people with physical disabilities. Over time it may admit more people with dementia, mental health conditions or complex behavioural support needs. Once that shift becomes part of the ordinary service, the registration details should not lag behind it.
A carer once summed this up in practical terms: “It changed bit by bit, then one day it was obvious the home was supporting a very different group from the one it started with.” That kind of drift is common. It is also easy to miss until a review, complaint or inspection brings it into view.
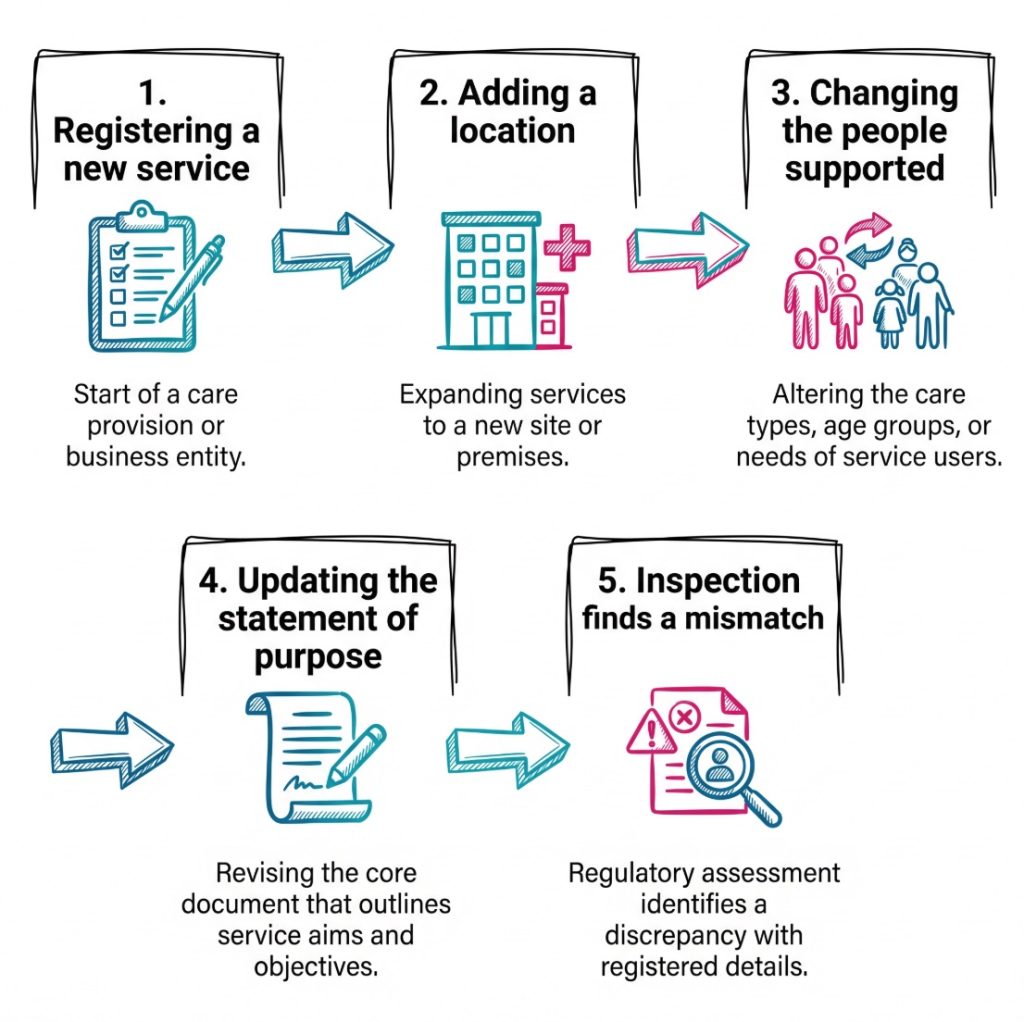
A useful way to think about review points is this:
- Registration stage: The provider sets out who the service is for when applying to register with CQC.
- New location: A new site needs its own accurate description of the people it will support.
- New regulated activity: Adding a regulated activity can change the shape of the service and the client group it serves.
- Change in referrals: A steady change in the kinds of placements being accepted may mean the service has outgrown its original description.
- Inspection or governance review: Internal audits or CQC findings may show that the service user bands no longer match the actual service.
Services for autistic people and people with a learning disability need especially careful thought. CQC has separate pre application guidance for these services, and wider policy sits alongside Right support, right care, right culture. The reason is plain enough. The service model itself needs to be right, not just the paperwork.
A service can deliver personal care and still be the wrong setting.
How do service user bands work in day to day service decisions?
Service user bands should shape decisions before a person moves in or starts receiving care. They are most useful at the referral and assessment stage, when a provider is deciding whether the service is a good fit.
A straightforward sequence helps here.
- Define the client group: The provider identifies the main group the service is built for. That description should be realistic and specific enough to guide decisions.
- Match the statement of purpose: The formal statement should describe the same service, using language that fits the registration record.
- Build the service around that group: Staffing, training, routines, the environment and risk systems should fit the people the service supports.
- Use the bands during admissions: A referral should be judged against the service model, not just against whether a bed or a rota slot is available.
- Review after change: If the client group shifts, the provider should revisit the statement of purpose, registration details and workforce plans.
That sequence can look different across settings.
In a care home, the question may centre on whether the environment fits the person. Does the service have the right layout, pace, peer group and staffing pattern for that client group?
In domiciliary care, the issue may be less about the building and more about staff competence, lone working, communication methods and risk management. Skills for Care workforce planning guidance is useful here because service design and staffing fit closely together. HSE guidance for health and social care and moving and handling guidance also show how the service model needs to line up with safe systems of work.
In a specialist residential service, especially one linked to autism or learning disability, the service model goes much deeper. The provider may need to show that support promotes choice, community inclusion, ordinary living and the least restrictive approach. Wider guidance from NHS England on learning disability and autism and NICE guidance on people’s experience in adult social care helps frame that broader picture.
On second thought, the real dividing line is not specialist versus non specialist. It is whether the service can show a coherent model for the people it says it supports.
A mini case study shows how the issue can unfold.
- Setting: A home care agency registered for older people, dementia and sensory impairment.
- Referral: The agency is asked to support a 28 year old autistic adult with significant communication needs.
- Immediate question: The package includes personal care, but is the service actually designed for this person’s main needs?
- Wider check: The agency looks at staff training, communication support, risk assessment, family liaison and whether its statement of purpose reflects this client group.
- Outcome: The decision turns on service fit, not just task lists.
That is where service user bands earn their keep. They help turn a broad regulatory category into a practical decision about suitability.
Where do service user bands fit with law, standards and roles?
Service user bands sit within the CQC registration system, but they also connect with several other parts of the legal and regulatory framework.
The first link is the statement of purpose. A provider must have one for each regulated activity it carries on, and it should stay accurate over time. That requirement comes from the Care Quality Commission (Registration) Regulations 2009.
The second link is the wider registration framework under the Health and Social Care Act 2008. A provider carrying on regulated activities needs to be registered with CQC. Registration is the legal foundation. Service user bands are one part of how the service is described within that system.
The third link is the fundamental standards under the 2014 regulations. The most relevant areas are usually person centred care, safe care and treatment, staffing and good governance. An outdated or misleading band may point to wider problems in one or more of those areas.
Other legislation shapes the same terrain. The Care Act 2014 sets the wider framework for adult care and support, including wellbeing, assessment and carers’ support. The Mental Capacity Act 2005 and its Code of Practice are relevant where decision making, capacity and best interests come into play. The Equality Act 2010 sits behind reasonable adjustments and fair access. Guidance from SCIE, including its work on safeguarding adults and the Care Act assessment and eligibility process, helps connect those duties to day to day practice.
Several roles need to keep a close eye on this.
- Registered provider: The provider is responsible for the service overall and for keeping registration details accurate.
- Registered manager: The manager needs to know what the service is registered to provide and how that affects admissions, staffing and oversight.
- Nominated individual: In an organisation, this role supports regulatory oversight and accountability.
- Referral or placement leads: These staff often sit at the point where service user bands turn into real decisions about fit.
- Commissioners and local authorities: They may influence placements, though the provider still carries responsibility for deciding whether the service is suitable.
Other bodies shape the wider picture. NHS England influences service models and pathways in health care. Skills for Care shapes workforce development in adult social care. HSE oversees workplace health and safety in health and social care settings. Different roles. One shared thread.
What are common mistakes with CQC service user bands?
The most common mistake is treating service user bands as a one off form filling task. Services change. Referral patterns change. Commissioners ask for different placements. Managers sometimes stretch the service to meet local demand. Once that happens, the original description may stop fitting the real service.
Another common mistake is choosing too many bands. A broad list can make the service sound flexible, but it can also make the description vague. If everything is included, the service’s real focus becomes hard to see.
There is also a mistake at the referral stage. Providers can end up judging referrals only by the tasks involved, such as personal care, medicines support or observation. That approach is too narrow. A service may be able to complete the tasks and still be the wrong setting for the person.
Confusion around overlapping needs causes problems too. A person may have several diagnoses, but the service user band should still reflect the main client group the service is built for. The detailed picture belongs in assessment and care planning.
Training can drift here as well. A service may say it supports a broad client group, but its induction, supervision and competency checks may still reflect the older model. The Care Certificate gives a baseline for new workers, but specialist groups often need more than baseline training.
A short checklist helps keep the basics clear.
- Check the main client group: The band should describe the core service, not every possible need seen from time to time.
- Check the statement of purpose: The service description should match the client group in clear language.
- Check staffing and training: Staff skills should fit the client group the service says it supports.
- Check the environment or delivery model: Buildings, routines or home care systems should reflect the needs of the people using the service.
- Check referral decisions: Admissions should be tested against service fit, not only against available capacity.
- Check review points: Growth, new contracts and inspection findings can all trigger the need for an update.
“The simplest test is whether the service on paper is the same service people receive.”
One final caution belongs here. Specialist depth and broad flexibility are not the same thing. A general service can support a wide range of people. A specialist service needs a clear model built around a defined client group. Mixing those ideas can lead to trouble.
Conclusion
CQC service user bands are a plain description of who a service is set up to support. They are part of registration. They are not a quality rating, and they do not rank people by need.
Used properly, they help keep the service honest. They connect the registration record with staffing, environment, admissions, care planning and governance. When those pieces line up, the service has a much clearer basis for safe and suitable care.
When they drift apart, problems follow. A service may begin to support people it is not really built for. Staff can be left working beyond the original model. The person using the service may end up in a setting that does not fit their age, communication style, lifestyle or support needs.
The practical next step is straightforward. Any provider, manager or reviewer looking at service user bands would compare the actual client group with the statement of purpose, the registration details and the real service model. If those three things match, the service description is likely to be in decent shape. If they do not, the gap needs attention.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.