
The four CQC ratings are Outstanding, Good, Requires improvement and Inadequate. The Care Quality Commission, known as CQC, uses these ratings to show how well a registered health or adult social care service is performing in England.
You will see these ratings linked to care homes, home care agencies, hospitals, GP practices, hospices, dentists, mental health services and supported living services where the provider carries on a regulated activity, such as personal care.
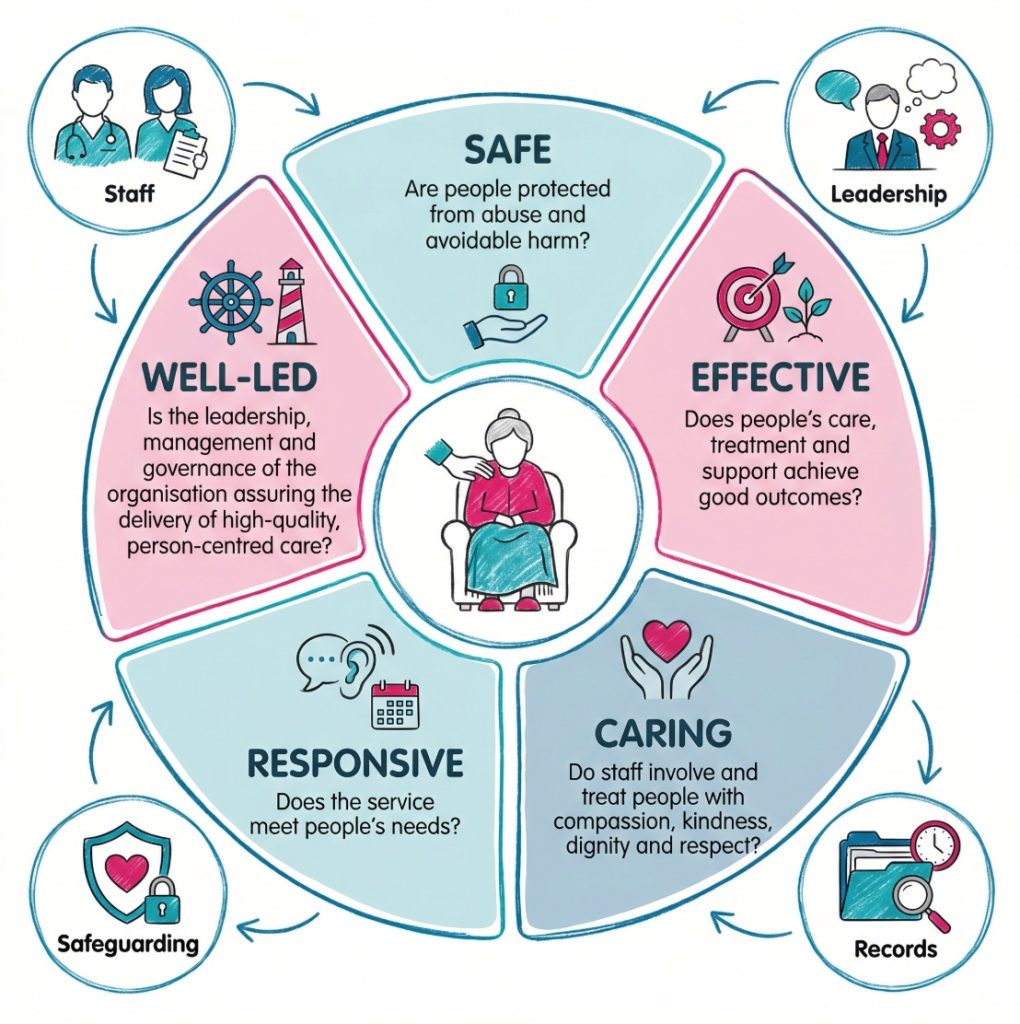
The ratings give a quick view of whether a service is safe, caring, effective, responsive and well-led.
The four ratings sit on a simple scale:
- Outstanding: The service is performing exceptionally well and shows strong evidence of high-quality care.
- Good: The service is performing well and meeting expected standards.
- Requires improvement: The service is not performing well enough and needs to make changes.
- Inadequate: The service is performing poorly and may have serious problems with safety, leadership or care quality.
CQC also uses percentage scores in newer assessment reports. These scores show where a service sits within a rating band. The current CQC score ranges are 88 to 100% for Outstanding, 63 to 87% for Good, 39 to 62% for Requires improvement, and 38% or lower for Inadequate. The official explanation is available on CQC ratings and scores.

A CQC rating is not just a label. It reflects how care feels, how risks are managed and how leaders check quality.
The rating should be read with the full CQC report. A service may be rated Good overall but still need to improve one area. Another service may be rated Requires improvement but may already be changing the way it works.
The rating gives the headline. The report gives the detail. The useful question is simple: what does this mean for the person receiving care?
| CQC rating | What it means | What this may look like |
|---|---|---|
| Outstanding | The service performs exceptionally well | Care feels personal, staff act early, leaders learn and improve |
| Good | The service performs well | Care is safe, respectful, organised and consistent |
| Requires improvement | The service needs to get better | Systems may be weak, records may be poor, or care may vary |
| Inadequate | The service performs poorly | People may face serious risks, poor care or weak leadership |
Why CQC ratings are important
CQC ratings help people compare services, read reports more confidently and ask better questions. Without them, it can be hard to judge whether a care home, home care agency or health service is well managed.
They also give a public view of quality. People receiving care, families, advocates, staff, managers, commissioners and health professionals can use the rating as a starting point. Providers are expected to show evidence that care is safe and well managed.
CQC looks at five main questions when assessing many services. These are explained on the five key questions CQC asks.
- Safe: People are protected from avoidable harm, abuse and poor care.
- Effective: Care supports people’s needs, goals and outcomes.
- Caring: Staff treat people with kindness, dignity and respect.
- Responsive: The service adapts to people’s needs, choices and concerns.
- Well-led: Leaders manage the service in a way that supports safe, high-quality care.
Care quality is rarely about one single issue. A care home may feel warm and friendly, yet medicines may not be managed safely. A home care agency may employ kind staff, but late or missed visits may leave people without support at the time they need it.
Daily work feeds into the bigger picture. Good recording, safe medicines practice, clear handovers, safeguarding reports and respectful communication can all contribute to the evidence that shows how safe and well-led a service is.
These are not background tasks. They affect the person receiving care.
Good notes are not paperwork for its own sake. They help the next worker see what has changed, what has been done and what still needs attention.
A strong rating can reassure people that a service is organised and person-centred. A weaker rating may raise questions about staffing, safety, leadership and improvement.
What Outstanding means
An Outstanding rating means a service is performing exceptionally well. The service does more than meet basic standards. It shows strong evidence that people receive high-quality, personalised and well-led care.
Outstanding care often shows up in everyday details. Staff know the person’s preferences, communication needs, life history, risks, strengths and goals. Care is shaped around the person, not around staff convenience.
In a care home, a person living with dementia may become anxious in a busy dining room. A weaker response might only record that the person was unsettled. A stronger response looks for the reason.
Staff may offer a quieter space, use familiar routines, involve family in life history work and adapt how they communicate.
That is real care planning. Not guesswork.
A home care service rated Outstanding may notice small changes quickly. A person may become quieter, eat less or walk less steadily. Care workers pass this on early, and the office may review the care plan, speak with family, contact the GP or involve another professional where suitable.
Leadership also tends to be strong. Registered managers and senior staff know what is happening because they listen, observe, audit and act. They do not wait for inspection to find problems.
Outstanding care often shows itself in small details: a noticed change, a familiar routine, a calm response and a service that learns quickly.
An Outstanding rating does not mean a service never makes mistakes. Care services deal with pressure, risk and complex human needs. The stronger sign is how the service responds when something goes wrong.
Good learning, honest communication and quick action can protect people from repeated harm.
People receiving Outstanding care may feel known, respected and involved. Families may feel staff communicate well. Staff may feel trusted, supported and confident to speak up.
What Good means
A Good rating means a service is performing well and meeting expected standards. It is a positive rating. It usually shows that people receive safe, effective and respectful care.
Good care should be consistent. A person should not receive good care only when a favourite staff member is on shift. The service should have systems that support safe care across different staff, visits, departments and days.
In a care home, a Good rating may show that staff know people well, medicines are handled safely, records are accurate, risks are reviewed and people are treated with dignity.
In a home care agency, it may show that visits are planned properly, staff arrive as expected, and concerns are passed on quickly.
Good does not mean perfect. A Good service may still be working on staff training, activities, digital records, communication or care planning. The rating means the service is working at a reliable level.
For staff, Good usually means expectations are clear. Staff know how to report safeguarding concerns, follow care plans, record changes, involve people in decisions, and raise risks with the right person.
They receive training, supervision and guidance.
A Good service often feels organised to staff. People know who to contact, what to record and what to do when something changes. Clear systems help staff act early.
For people receiving care, Good should feel dependable. Kindness helps, but it is not enough on its own. Safe systems, accurate records, strong communication and good leadership are also needed.
A Good rating can slip if leaders stop checking quality. Services can decline when staffing becomes unstable, audits weaken, complaints are ignored or records fall behind.
Strong Good services keep checking care before problems grow.
What Requires improvement means
A Requires improvement rating means a service is not performing as well as it should. It does not always mean people are in immediate danger, but it does mean CQC has found areas that need to improve.
The reasons can vary. A service may have caring staff but poor records. Care may be safe in some areas and inconsistent in others. Policies may exist, but there may be little proof that they shape daily work.
A home care agency may receive Requires improvement if some visits are late, records are incomplete or managers do not monitor missed calls properly.
A care home may receive this rating if risk assessments are out of date, staff training is patchy or incidents are not reviewed well enough.
Small gaps can grow. Poor records may mean staff miss changes in health. Weak audits may allow unsafe routines to continue. Inconsistent training may leave staff unsure about safeguarding, infection prevention, medicines or mental capacity.
Governance is an important word here. It means the systems and processes a service uses to assess, monitor and improve the quality and safety of care.
This can include audits, staff supervision, incident reviews, complaints analysis, risk monitoring and action plans. Skills for Care offers helpful material on improving your CQC rating, especially for adult social care services.
When a service receives Requires improvement, leaders usually need a clear improvement plan that matches the concerns found in the report. The plan should say what will change, who will lead each action, how progress will be checked and how people will stay safe while changes are made.
For people receiving care, this rating may raise fair questions. The full report helps show whether the concern relates to records, staffing, safety, leadership or direct care.
What Inadequate means
An Inadequate rating is the lowest CQC rating. It means the service is performing poorly and may have serious problems with safety, care quality, leadership or people’s rights.
An Inadequate rating can be linked to serious or repeated failures. These may include unsafe medicines management, poor safeguarding, weak leadership, too few suitably trained staff, poor infection prevention, unsafe premises, poor records or failure to respond when people’s needs change.
The impact can be direct. A person may feel unsafe, ignored, rushed or unsupported. Their dignity may not be protected.
They may not receive the care described in their care plan. Risks such as falls, choking, pressure damage, dehydration or missed medicines may not be managed well enough.
In a care home, an Inadequate rating could involve repeated falls that are not properly reviewed. In a home care agency, it could involve missed visits where people depend on staff for food, medicines or personal care.
In a hospital ward, it could involve unsafe staffing, weak infection control or delays that affect patient safety.
CQC’s adult social care guidance says services rated inadequate overall go straight into special measures. If a service is rated inadequate for one of the five key questions, CQC will inspect it again within six months of the report being published.
If it remains inadequate in any key question at that second inspection, it will enter special measures.
Staff may find an Inadequate rating upsetting. Many staff work hard in difficult conditions. A poor rating can also show wider problems with systems, staffing, training, culture and leadership.
An Inadequate rating should never be treated as a paperwork issue. It can mean people are exposed to avoidable harm.
How CQC decides a rating
CQC decides ratings by looking at evidence about care quality and safety. It does not rely only on what a service says about itself. It looks for signs that good care is happening for people.
The five key questions shape the assessment: Safe, Effective, Caring, Responsive and Well-led. They help CQC build a rounded picture of the service.
CQC groups evidence into six categories:
- People’s experience: This looks at what people say about their care and whether care feels safe, respectful and responsive.
- Feedback from staff and leaders: This includes what staff and leaders say about training, culture, systems and risks.
- Feedback from partners: This can include views from other professionals or organisations that work with the service.
- Observation: This can include what assessors see during visits, where observation is part of the assessment.
- Processes: This includes systems such as care planning, audits, complaints, staffing checks and risk management.
- Outcomes: This looks at the results and impact of care for people.
CQC also uses quality statements within its current assessment framework. These sit under the five key questions and describe what providers, commissioners and system leaders should be working towards.
The rating should reflect a range of evidence. Serious safety concerns can carry heavy weight. Unsafe medicines practice, for instance, may strongly affect the rating, even if staff are caring in other ways.
Inspectors do not only read policies. They look for signs that those policies have reached the person receiving care.
How ratings work in real care settings
CQC ratings influence how services are viewed and how they improve. A rating can affect public confidence, staff morale, referrals, contracts and relationships with local authorities or health partners.
Take a residential care home rated Good overall. The report says staff are kind, medicines are managed safely and people feel listened to. It also says activities could be more personalised.
The service is performing well, but leaders have a clear area to improve.
Now take a home care agency rated Requires improvement. Staff may be caring, but the provider may not monitor visit times well enough. Some care notes may be incomplete.
People may like their care workers, yet the systems behind the care may not be reliable enough.
In a GP practice, Requires improvement may relate to access, safety checks, governance or complaints handling. Individual clinicians may give good care, but the practice may need stronger systems to manage risk.
In supported living, CQC may focus on the personal care being provided. The rating may reflect whether staff understand communication needs, whether people have choice and control, and whether risks are managed without removing independence.
In hospitals, ratings may vary between departments. Urgent and emergency care may have a different rating from surgery, maternity, mental health or medical care. This is why the specific service rating can be more useful than the wider organisation rating.
The headline rating gives the summary. The report explains the evidence. Read both where possible.
Where CQC ratings apply
CQC ratings apply to many registered health and adult social care services in England that carry out regulated activities. A regulated activity is a type of care, treatment or support that requires CQC registration when the legal conditions apply.
People can search for services through CQC find care services. This can show inspection reports, ratings and details about registered providers and locations.
Common settings include:
- Care homes: Ratings may cover personal care, nursing care, medicines, staffing, dignity, activities, safeguarding and leadership.
- Home care agencies: Ratings may cover call times, missed visits, care planning, staff training, medicines support and communication.
- GP practices: Ratings may cover patient access, safety systems, leadership, clinical governance and responsiveness.
- Hospitals: Ratings may cover services such as surgery, urgent and emergency care, maternity, mental health and medical care.
- Hospices: Ratings may cover end of life care, symptom support, family involvement, dignity and leadership.
- Dental services: CQC regulates dental services, although rating arrangements can differ from some other services.
- Supported living services: CQC may regulate the care people receive, such as personal care, but it does not regulate the person’s accommodation in the same way as a care home.
The supported living point is often misunderstood. A person may live in their own home and receive care or support from a registered provider. CQC’s role depends on the regulated activity being carried on, not simply on the housing model.
Not every care-related service has a CQC rating. Some services may not fall within CQC registration requirements. Others may be new and not yet rated.
The setting alone does not tell the whole story. The regulated activity explains whether and how CQC is involved.
What standards and legislation link to CQC ratings?
CQC ratings are linked to legal duties, regulations and standards. These set expectations for safe, respectful and well-managed care.
The main legal framework includes the Health and Social Care Act 2008, which established CQC as the regulator for health and adult social care in England. CQC explains its powers on legislation and CQC powers.
A central set of regulations is the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014. These include the fundamental standards. These standards set the baseline for care and treatment that registered services are expected to meet.
The legislation is available through the Regulated Activities Regulations 2014.
Important areas within the regulations include:
- Person-centred care: Care should reflect the person’s needs, choices and circumstances.
- Dignity and respect: Staff should protect privacy and treat people respectfully.
- Consent: People should be involved in decisions where they can be.
- Safe care and treatment: Risks should be assessed, reduced and reviewed.
- Safeguarding: People should be protected from abuse, neglect and improper treatment.
- Staffing: There should be enough suitably skilled and supported staff.
- Good governance: Providers should check quality and act when standards slip.
- Complaints: Concerns should be listened to and handled properly.
- Duty of candour: Providers should be open and honest when certain safety incidents happen.
Other laws also shape care quality. The Mental Capacity Act 2005 is important when a person may lack capacity to make a specific decision.
Capacity means the ability to understand, retain and weigh up information relevant to a specific decision, and to communicate that decision at the time it needs to be made. Information about the Act is available through Mental Capacity Act guidance.
The Care Act 2014 is relevant to adult safeguarding. It deals with care, support and protection from abuse or neglect. The Act is available through the Care Act 2014.
These laws affect daily care. They shape how staff gain consent, manage risk, record decisions, involve people, report concerns and protect dignity.
How each rating can affect people receiving care
CQC ratings affect people because they reflect the service they may rely on every day. This can include support with personal care, medicines, mobility, communication, meals, continence, mental health or decision-making.
A person using an Outstanding service may experience care that feels thoughtful and flexible. Staff may notice small changes early, encourage independence and adapt support around the person’s preferences.
A person using a Good service should usually receive reliable and respectful care. Their care plan should reflect their needs. Staff should know how to support them safely.
A person using a Requires improvement service may still receive kind care, but the experience may be less consistent. One staff member may know their needs well, while another may not.
Records may not always be up to date. Communication may be weaker than it should be.
A person using an Inadequate service may face a higher risk of poor care or harm. This could include missed care, unsafe moving and handling, poor medicines support, weak safeguarding or lack of dignity.
Families and advocates may also look at the rating. A strong rating can offer reassurance. A weaker rating may lead them to ask how risks are being managed and what has changed since the last report.
Staff are affected too. A strong rating can build pride and confidence. A weaker rating can feel stressful, but it can also identify what needs to change.
A rating is most useful when it is connected to real life: meals, medicines, call times, dignity, safety and the way staff listen.
What staff should know about the 4 ratings
Staff do not need to know every technical part of CQC methodology. They do need to know how their daily practice links to ratings.
CQC ratings are not only about managers, policies or inspection visits. Everyday care shapes the quality of the service. Communication, recording, reporting, listening and safe support all affect people’s experience.
Staff should know that:
- Ratings reflect people’s lived experience: CQC looks at how care feels and works for people, not only what the provider says.
- Records support safe care: Poor records can lead to missed information, repeated mistakes or unsafe decisions.
- Speaking up supports safety: Staff should raise concerns through the right local route when something feels wrong or unsafe.
- Person-centred care should be visible: Care plans and daily notes should show the person’s needs, choices and preferences.
- Leadership affects daily work: Good managers support staff to deliver safe and consistent care.
- Improvement belongs to the whole team: Staff at every level can notice risks, suggest changes and support better outcomes.
A care worker supporting breakfast is not only completing a task. They may be supporting nutrition, dignity, choice, communication and risk management.
If the person eats less than usual, coughs while drinking or seems more confused than usual, staff should record the change and share it with the right person according to local procedures.
A nurse managing medicines is not only doing a medicines round. They are supporting safe care and treatment. Accurate records, safe storage, error reporting and clear communication all affect quality.
A team leader completing an audit should not treat it as a paper exercise. An audit should help the service see whether care is safe and where staff need support.
Small actions build safer care.
How to read a CQC rating step by step
A CQC rating is easier to read when broken down. This can help learners, staff, families and people comparing services.
A useful step-by-step approach is:
- Step 1: Check the overall rating: Start with the main rating: Outstanding, Good, Requires improvement or Inadequate.
- Step 2: Look at the five key questions: Check the ratings for Safe, Effective, Caring, Responsive and Well-led.
- Step 3: Read the main findings: Look for what CQC found about care, leadership, staffing, records and risk.
- Step 4: Notice any regulation breaches: A breach may show that the provider did not meet a legal requirement.
- Step 5: Check the date: Older reports may not show the current service.
- Step 6: Look for patterns: One issue may be isolated, but repeated concerns can suggest wider problems.
- Step 7: Ask focused questions: Use the report to ask about medicines, staffing, care planning, safeguarding or improvement.
- Step 8: Look for evidence of change: Improvement should show through care records, audits, training, feedback and daily routines.
If a report says medicines audits were poor, the next question is about what changed and how leaders know the new system works.
If a report says care plans were not updated, look for how staff now review care plans when people’s needs change.
This approach stops the headline rating from doing all the work. It also helps staff connect inspection findings with daily care.
Examples of CQC ratings in different settings
The same four ratings can look different depending on the setting. Care risks and responsibilities vary.
In a care home, Outstanding may involve excellent dementia care, strong family involvement, meaningful activities, safe medicines management and staff who know people well. Requires improvement may involve out-of-date care plans or weak monitoring of falls.
In a home care agency, Good may mean staff arrive on time, stay for the planned visit, understand people’s routines and report changes quickly. Inadequate may involve missed calls, poor office communication and weak systems for checking whether people received care.
In a GP practice, Good may mean safe systems, effective follow-up, responsive care and clear leadership. Requires improvement may relate to access, safety checks, complaints handling or governance.
In a hospital ward, ratings may reflect staffing, infection prevention, patient dignity, discharge planning, medicines safety and clinical oversight. A ward may be caring but still need improvement if safety systems are inconsistent.
In a supported living service, CQC may focus on personal care. A Good service may help people make choices, manage risks positively and stay involved in the community. A weaker service may fail to adapt support when people’s needs change.
In a hospice, ratings may consider symptom support, end of life care, emotional support, family involvement and respect for people’s wishes.
The setting changes the detail, but the rating still comes back to the same broad questions: are people safe, listened to, cared for properly and supported by a well-led service?
Common mistakes when reading CQC ratings
People can misunderstand CQC ratings if they only look at the headline word. The rating is useful, but context gives the fuller picture.
Common mistakes include:
- Thinking Good means perfect: A Good service can still have areas to improve.
- Thinking Requires improvement always means unsafe: It means weaknesses exist, but the level of risk depends on the evidence.
- Ignoring the key question ratings: The overall rating can hide important detail about Safe, Effective, Caring, Responsive or Well-led.
- Not checking the report date: A service may have improved or declined since the report.
- Focusing only on paperwork: Records are important, but people’s experiences and staff practice are also important.
- Assuming one rating covers every part of a large service: Hospitals and large providers may have different ratings for different services or locations.
- Forgetting the person’s experience: Policies and audits are useful only when they lead to safe, respectful and responsive care.
A fair challenge is that ratings cannot show every detail of a service. That is true. A rating is a summary, not a record of every visit, shift or conversation.
The answer is to read the report, check the date and look at the evidence behind the judgement.
Another mistake is thinking CQC ratings only count during inspection. The practice behind a rating is built every day. Care notes, handovers, risk reviews, supervision, complaint responses and safeguarding decisions all contribute to quality.
Inspection is not separate from care. It should reflect what people experience when staff support them.
How services may improve after a weaker rating
When a service receives Requires improvement or Inadequate, improvement should be planned, monitored and evidenced. Vague promises are not enough.
A service will usually need to review the CQC report carefully. Leaders need to identify the main concerns and decide what needs urgent attention. Some issues may need immediate action, especially where people are at risk.
An improvement plan may include:
- Clear actions: The plan should say exactly what will change.
- Named responsibility: Each action should have someone responsible for leading it.
- Timescales: The service should set dates for review and completion.
- Evidence: Leaders should collect proof that improvement is happening.
- Staff involvement: Staff should be asked what helps or blocks safe practice.
- People’s feedback: People receiving care should be asked whether care has improved.
- Regular review: Leaders should check whether changes are working in daily care.
Poor medicines management is a good example. A service may retrain staff, improve storage, introduce daily checks and complete regular audits. Training alone may not solve the problem.
Leaders also need ways to check whether staff are following safer practice.
If CQC found weak care planning, staff may need to review each person’s care plan with them and, where appropriate, their family or advocate. The plan should reflect current needs, risks, communication, preferences and goals.
Good improvement work should show in daily care. People should notice better communication, safer routines and more consistent support.
Why leadership shapes CQC ratings
Leadership strongly affects CQC ratings because leaders shape culture, staffing, systems and accountability. This is why Well-led is one of CQC’s five key questions.
Good leadership does not only mean having a manager in post. It means leaders know the service, listen to people, support staff and act when something is not right.
A well-led service should be able to answer clear questions:
- How do we know people are safe? Leaders should use audits, feedback, incidents, observations and safeguarding information.
- How do we listen to people? People’s views should influence care planning and service improvement.
- How do we support staff? Staff should receive training, supervision, guidance and time to raise concerns.
- How do we learn from mistakes? Incidents and complaints should lead to reflection and change.
- How do we know improvement is working? Actions should be tested through real care, not only recorded on a plan.
Poor leadership can affect every other area. If leaders do not monitor risks, staff may miss important changes. If leaders ignore concerns, people may lose trust.
If leaders focus only on documents, care can become task-based rather than person-centred.
Good leadership also supports staff confidence. Staff should feel able to speak up when something is unsafe or unclear. Openness helps stop small concerns becoming serious problems.
For people receiving care, leadership may not always be obvious. They still feel its effects through organised care, respectful staff, quick responses and clear communication.
What to look for beyond the rating
A CQC rating is helpful, but the service still needs to suit the person’s individual needs. A rating gives a starting point. The full report, conversations and visits add detail.
Useful areas to consider include:
- The person’s needs: This includes health, communication, culture, routines, risks and preferences.
- Care planning: People should be supported to have a say where possible.
- Concerns and complaints: Feedback should be welcomed and acted on.
- Staff support: Training, supervision and staff stability can affect care quality.
- Family and advocate communication: This can be important when the person wants others involved.
- Risk review: Risk assessments should change when the person’s needs change.
- Recent improvement: This is especially important after a Requires improvement or Inadequate rating.
For a family looking at a care home for someone living with dementia, the rating is only one part of the picture. They may also want to ask how staff support distress, personalise routines and reduce isolation.
For home care, the detail may be different. Visit monitoring, late-call procedures and how care workers are matched to people’s needs may be more relevant.
When a care home is being considered, NHS guidance on care homes can also help explain care options and questions to consider.
A rating should support choice. It should not replace careful questions, visits and conversations.
Practical checklist for CQC ratings
A simple checklist can help when reading a CQC report or comparing services.
- Overall rating: Check whether the service is Outstanding, Good, Requires improvement or Inadequate.
- Five key questions: Look at Safe, Effective, Caring, Responsive and Well-led separately.
- Report date: Check when the service was assessed or inspected.
- Main concerns: Look for repeated themes, especially around safety, staffing, leadership or safeguarding.
- Strengths: Notice what the service does well, especially where people describe good care.
- Regulation breaches: Look at any breaches because they show where CQC found the provider had not met a regulation.
- Improvement evidence: Look for signs that the service has acted since the report.
- Fit for the person: Think about the person’s needs, communication, routines, risks and preferences.
- Staff culture: Look for signs that staff are supported, trained and able to speak up.
- Leadership: Check whether managers know the service and act on problems.
This checklist helps turn the rating into something useful. It keeps the focus on people, staff and the quality of care.
Conclusion
The four CQC ratings are Outstanding, Good, Requires improvement and Inadequate. They give a clear way to describe how well a health or adult social care service is performing in England.
Outstanding shows exceptional practice. Good shows the service is performing well. Requires improvement means the service needs to get better. Inadequate means there are serious concerns and urgent improvement may be needed.
These ratings are about real people, not just inspection reports. They connect to safety, dignity, choice, rights, communication, leadership and daily care.
The ratings become clearer when they are linked to real care. What does the rating mean for the person receiving support? What does it mean for staff on shift? What does it say about leadership, governance and improvement?
A strong service should not only aim for a positive rating. It should aim to provide care that is safe, kind, responsive and well-led every day.
That is the standard.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.