
Cultural humility is an ongoing way of working in which health and social care staff reflect on their own assumptions, recognise power imbalances, and learn from each person’s identity, values and lived experience instead of assuming they already know what those mean.
The phrase came from Melanie Tervalon and Jann Murray García, who described it as lifelong self evaluation, self critique and close attention to unequal relationships in care. It still feels current. Staff cannot learn a list of facts about a group and expect that list to explain the next person they meet.
Culture is wider than ethnicity or religion. It may include disability, age, sexuality, gender identity, language, education, trauma, family roles, migration history, class and community life. It can also shape how a person sees illness, privacy, touch, risk, food, faith, family involvement and independence. Two people from the same background may want very different care. That is the point.
This sits very close to person centred care. CQC guidance on Regulation 9 says care and treatment should be personalised and based on the person’s needs and preferences. The NMC Code says nurses, midwives and nursing associates must treat people as individuals, listen to their preferences and work in partnership with them. Social Work England’s professional standards push in the same direction, and the Care Certificate standards place equality, diversity, inclusion, human rights and person centred values early in induction for new workers.
“Treat people as individuals and uphold their dignity.”
That line from the NMC Code fits this subject because cultural humility begins with the person, not the label.

Why Cultural Humility Has a Place in Everyday Care
Health and social care run on unequal relationships. Staff have access to records, systems, referrals, assessments, professional language and care plans. The person receiving care may be unwell, distressed, tired, dependent on services or worried about being judged. Good intentions do not remove that imbalance. Busy shifts do not help.
If workers miss that imbalance, they may speak for the person rather than with them. Silence can be read as agreement. A nod can be taken as consent. A relative may be allowed to take over because it seems quicker. Small moments. Big effect.
Cultural humility gives staff a steadier way to work. It asks them to look at their own habits as well as the person’s needs. That includes assumptions about pain, family roles, gender, food, religion, communication, mental health, risk and capacity. A care plan may look tidy on paper and still fail by tea time if it does not fit the person’s life.
The legal and professional backdrop supports this clearly. The Equality Act 2010 protects people from discrimination linked to protected characteristics. The Human Rights Act 1998 requires public authorities to act compatibly with protected rights. The Mental Capacity Act 2005 starts from the presumption of capacity and says a person is not to be treated as unable to decide simply because they make an unwise decision. The Care Act 2014 adds the duty to promote individual wellbeing. Cultural humility supports sharper judgement here because it helps staff separate difference from inability and disagreement from incapacity.
“Listen to people and respond to their preferences and concerns.”
That line from the NMC Code says a lot in plain language. Listening changes care.
There is a fair counter point. Workers still need background knowledge. It would be careless to ignore known patterns in health inequality, discrimination or communication barriers. A caveat here is that background knowledge should shape the questions, not replace them.
What Makes Cultural Humility Different from Cultural Competence
Cultural humility is often placed alongside cultural competence. The two overlap, though they do not produce the same kind of practice.
Cultural competence usually refers to the knowledge and skills needed to work with people from different backgrounds. Parts of that are useful. Staff need awareness of discrimination, communication barriers, social inequality and the ways these affect care. Training can reduce obvious mistakes. It can also give people a stronger starting point.
Trouble starts when competence is treated like a finish line. A worker may begin to think they understand a person because they know something about a group. That can make practice look informed while becoming less curious. Once curiosity drops, assumptions move in. The result can be efficient and well meant, yet still wide of the mark.
Cultural humility resists that drift. It keeps the worker in a learning position. Knowledge still counts, but it does not outrank the person’s own account of their life. Skills for Care’s work on person centred approaches, SCIE’s strengths based approach resources, and NICE guidance on shared decision making all support this more grounded way of working.
| Approach | Main focus | Main risk | Better question |
|---|---|---|---|
| Cultural competence | Building knowledge about groups and difference | Overconfidence and stereotyping | What should I know before I begin this conversation? |
| Cultural humility | Reflection, curiosity, power and individual experience | Reflection without action | What does this person need from me now, and what assumptions do I need to check? |
A few examples show the difference more naturally.
- Competence led response: “Families from this background usually want to be involved.” This may sound informed, but it can push the individual to one side.
- Humility led response: “Who would you like involved in this conversation?” This keeps the person at the centre.
- Competence led response: “I have had training on this community.” Training helps, though it does not give a full picture of one person’s life.
- Humility led response: “I have some background knowledge, and I still need to hear what this means for you.” That leaves room for the real conversation.
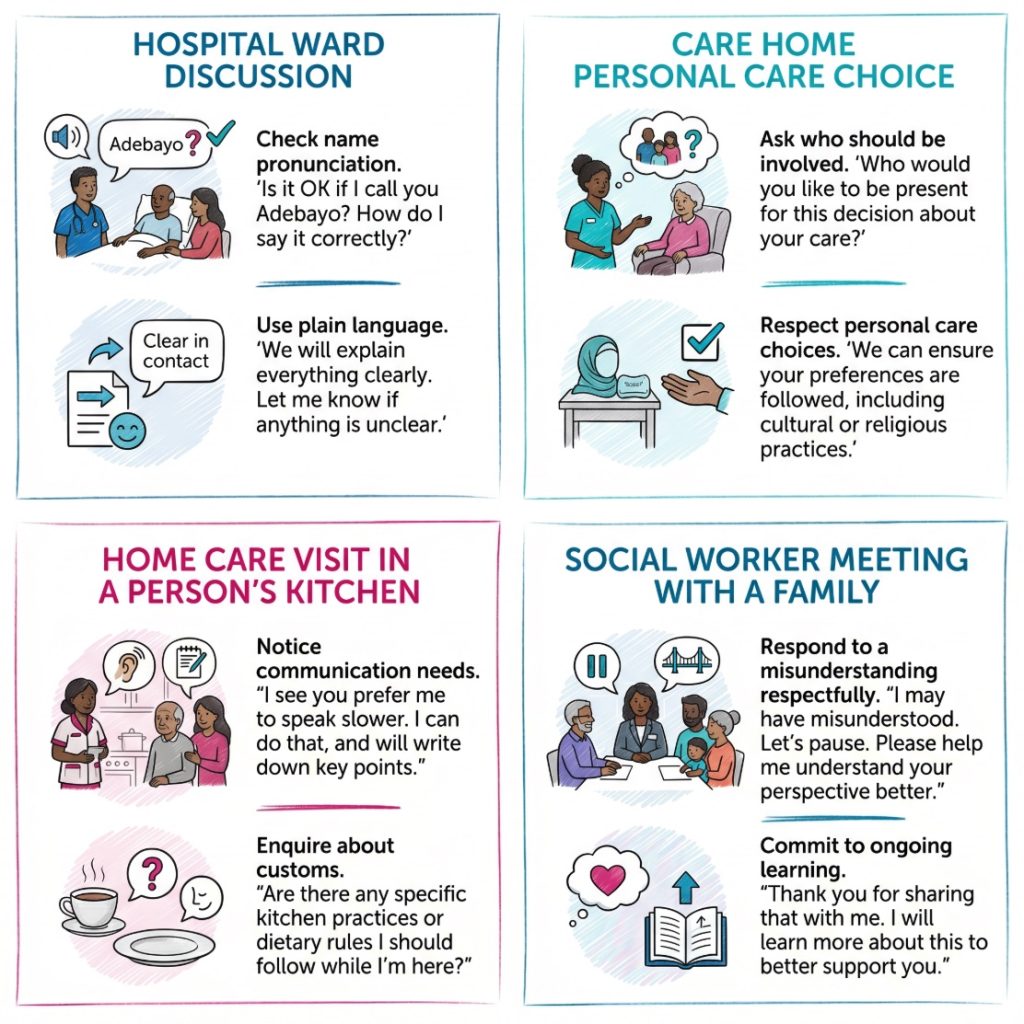
How Cultural Humility Shows Up in Real Settings
Cultural humility is easiest to spot in ordinary moments. It shows in how staff greet people, explain choices, check names, ask about communication support, involve relatives and respond when they get something wrong. Nothing flashy. Just careful work.
On a hospital ward, a nurse may notice that a patient says yes to everything but looks unsure. A culturally humble response would not stop at the yes. It would check what the patient has understood, whether the pace is too fast, whether an interpreter is needed, or whether the patient wants someone present for the discussion. NICE on shared decision making supports this joint approach to decisions, and the Accessible Information Standard reinforces the need to make information usable, not merely available.
In a care home, the same principle may affect food, visiting, privacy, worship, touch, personal care, daily routine or who is involved in reviews. CQC guidance on treating people as individuals refers to personal, cultural, social and religious needs, as well as communication and choice. One resident may want strong family involvement. Another may want privacy. One person may accept routine support from any member of staff. Another may find mixed gender personal care very distressing. Assumptions flatten all of that.
Home care adds another layer because the worker is entering someone else’s space. A rushed, task based visit may complete the checklist and still leave the person feeling handled rather than supported. A more careful approach may include checking household routines, privacy, family boundaries and what respectful support looks like in that home. The Care Act 2014 is relevant here because care and support are tied to wellbeing, daily life and the person’s own circumstances, not only to service tasks.
Mental health, learning disability services and social work often bring extra complexity. Silence may be read as non engagement when it is really fear. Strong family involvement may be read as pressure when it is chosen support. Previous poor treatment by services may shape how a person responds to professionals now. Social Work England places clear emphasis on dignity, partnership and respect for lived experience.
A support worker might put it more simply: “You only find out what helps when you stop assuming the file tells you everything.” That rings true because care records rarely hold the whole picture.
“Work in partnership with people.”
That phrase from the NMC Code is brief and direct. Partnership is the work.
When Cultural Humility Is Most Relevant
Cultural humility should not be kept for rare or sensitive conversations. It belongs across the whole care journey. Certain moments bring it into sharper focus.
The first assessment is one of them. Early assumptions settle quickly. Once a worker has labelled a person as difficult, passive, non compliant or over reliant on family, that label can follow the rest of the care plan. A calmer, more curious first conversation can prevent a good deal of poor practice later.
Consent and decision making are another obvious area. People may nod along to avoid embarrassment, to appear polite, or because the language feels too technical to challenge. Communication support can change the whole picture. The Accessible Information Standard says providers and commissioners of NHS and publicly funded adult social care services should make sure disabled people and people with impairments or sensory loss can access and understand information and receive the support they need to use services.
Review points deserve attention too. Needs, values and priorities shift over time. A person who wanted family present last year may want more privacy now. Someone who managed written information before may now need a different format. The Accessible Information Standard requirements set out a cycle of identifying, recording, flagging, sharing, meeting and reviewing communication needs. That fits neatly with cultural humility because it treats people’s needs as active, not fixed.
Difficult moments often expose the deeper issues. Complaints, tension with relatives, missed appointments or repeated misunderstanding may reflect a poor fit between the service and the person’s life rather than simple refusal. That does not mean the service is always at fault. It does mean the first explanation should not always be blame.
A family carer might describe this in plainer terms: “Mum wasn’t refusing help. She just needed staff to explain things in a way that made sense to her.” That sort of comment comes up often in care reviews and complaints work. It points to communication, pace and respect rather than defiance.
Useful trigger points include:
- Assessment: First impressions often shape everything that follows.
- Consent: Agreement is not the same as clear, informed choice.
- Care planning: A plan should work in the person’s real life, not only in the service file.
- Review: Old assumptions can stay in notes long after they stop being true.
- Conflict: Tension often exposes hidden assumptions or weak communication.
How Staff Can Build Cultural Humility Step by Step
Cultural humility develops through repeated habits. It is not a one day course and it does not arrive fully formed.
A workable sequence starts before the conversation begins. A worker can pause and notice the assumptions already in play. These may be about family, religion, communication, behaviour, risk, gender or capacity. That brief pause can be enough to change the tone of the whole exchange.
Next comes the conversation itself. Open questions leave room for the person’s own account. Careful listening helps staff hear what safety, dignity, privacy, family, independence or faith actually mean for that person. The Care Certificate standards, especially the standards on equality, diversity, inclusion, human rights and person centred care, support that way of working from the start of a person’s induction into care.
Communication then needs checking properly. Nodding is weak evidence of understanding. A stronger check is whether the person can explain the plan back in their own words or say which part is unclear. NICE shared decision making guidance supports joint decisions based on evidence and the person’s own preferences, beliefs and values, while NHS England’s Accessible Information Standard supports practical adjustments such as large print, email, a quieter room or communication support.
The work does not stop at the conversation. Staff need to record what actually helps, share relevant information lawfully with colleagues, and revisit it later. Reflection also counts. On second thought, reflection only helps if it leads to a changed response next time. SCIE’s strengths based resources are useful here because they keep the focus on the person’s own life, networks and priorities rather than on deficits alone.
A short case study makes this concrete. A domiciliary care worker supports an older man after discharge from hospital. He keeps refusing the breakfast offered and seems withdrawn. A task based reading of the situation might record poor appetite and low engagement. A more culturally humble response checks whether the food is familiar, whether the timing fits his routine, whether he has understood the discharge advice, and whether he would rather eat with a family member later. Same visit. Different outcome.
Useful steps include:
- Pause first: Before the conversation starts, notice the assumptions already in play.
- Ask open questions: Good questions leave room for the person’s own account rather than forcing them into a script.
- Check communication properly: Nodding is not enough. Clear communication may require a different pace, format or support.
- Share choices where possible: Joint decisions work better when options, limits and likely effects are explained plainly.
- Record what actually helps: Practical details should be captured and reviewed rather than left to memory.
- Reflect afterwards: A brief review can show what assumptions slipped in and what needs to change.
Where Law, Standards and Professional Bodies Connect to the Topic
Cultural humility is not the title of a single Act or regulation. It runs through the legal and professional framework that shapes good care.
The Equality Act 2010 is relevant because it protects people from discrimination linked to protected characteristics. That includes age, disability, race, religion or belief, sex and sexual orientation. In care settings, the practical question is often whether ordinary routines exclude or disadvantage people without anyone noticing.
The Human Rights Act 1998 is relevant because public authorities must act compatibly with protected rights. In health and social care, this often connects with dignity, private life, family life and freedom of thought or belief. The Mental Capacity Act 2005 is central when staff are making decisions with or for people who may have impaired decision making ability. Its principles warn against jumping too quickly from unusual choices to a finding of incapacity.
The Care Act 2014 also belongs here because it placed wellbeing, prevention and the wider shape of a person’s life at the centre of adult care and support. That fits closely with cultural humility, which asks staff to look beyond routine service delivery and pay attention to the person’s own priorities and context. CQC guidance on Regulation 9 brings the person centred side into sharp focus, while CQC guidance on treating people as individuals adds detail around identity, communication and personal, cultural, social and religious needs.
Professional bodies reinforce the same picture.
- NMC: The Code requires staff to treat people as individuals, listen to preferences, work in partnership and uphold dignity.
- Social Work England: Professional standards emphasise rights, strengths, dignity, privacy and trust.
- Skills for Care: Person centred approaches support workforce development that keeps the person at the centre.
- Care Certificate: The standards place equality, diversity, inclusion, human rights and person centred working at the heart of early learning.
- SCIE: Strengths based resources support work that sees people as more than their needs.
- NICE: Shared decision making guidance sets out a joint process based on evidence and the person’s own preferences and values.
- NHS England: The Accessible Information Standard supports accessible communication in NHS and publicly funded adult social care services.
Taken together, these sources point in one direction. Care should be individual, respectful, accessible and shaped with the person rather than delivered to them.
Common Mistakes, Practical Takeaways and a Short Checklist
The most common mistake is to confuse cultural humility with politeness. Good manners help, though they do not deal with power, bias or poor assumptions.
Another common slip is relying too heavily on general cultural knowledge. Group level information can help frame a conversation, but it should never replace that conversation. A worker who thinks they already know the answer often stops asking the right questions.
Communication is another weak spot. Services sometimes treat it as a detail rather than a core part of safe care. That is a serious error. If the person cannot access or use the information given, consent, planning and review are all weakened. The Accessible Information Standard and NICE’s work on shared decision making both underline this point.
Defensiveness after feedback causes trouble too. A worker who becomes protective when corrected is less likely to learn from the moment. Brief pause. Then repair. Team culture shapes this as much as individual attitude. HSE guidance on bullying and harassment is not social care guidance in the strict sense, but it is still relevant to workplace culture because staff are less likely to reflect honestly in teams where people feel blamed or shut down.
Common mistakes include:
- Assuming equality means identical treatment: Fair care may require different support for different people.
- Letting relatives take over without checking: Family involvement should reflect the person’s wishes, not service convenience.
- Using jargon and then moving on: Technical language can shut people out of decisions very quickly.
- Treating silence as consent: Quiet agreement may hide confusion, fear or fatigue.
- Labelling someone non compliant too quickly: A plan that does not fit the person’s life may fail for reasons that have little to do with motivation.
- Recording preferences once and never reviewing them: Needs and wishes can change over time.
A short checklist helps keep the topic grounded.
- Identity: Has the person been asked how they want to be addressed and what parts of identity are relevant to care?
- Communication: Has the service checked what format, pace or support the person needs?
- Choice: Has the person been given real options where options exist?
- Involvement: Has the service checked who the person wants involved in decisions?
- Reflection: Has the worker considered what assumptions shaped the conversation?
- Review: Have recorded needs and preferences been updated when circumstances changed?
Conclusion
Cultural humility is a disciplined way of staying open. It asks staff to keep learning, check their own assumptions and treat the person’s account of their life as central to good care. It is not vague. It shows up in names, questions, consent, communication, privacy, family involvement, capacity decisions and care planning.
It also fits squarely with the standards already shaping health and social care in England. CQC Regulation 9, the NMC Code, Social Work England standards, the Equality Act 2010, the Human Rights Act 1998, the Mental Capacity Act 2005, the Care Act 2014, NICE shared decision making guidance, SCIE strengths based resources and the Accessible Information Standard all point towards care that is individual, accessible and respectful.
The phrase itself may sound academic. The work is not. It lives in ordinary care, one interaction at a time.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.