
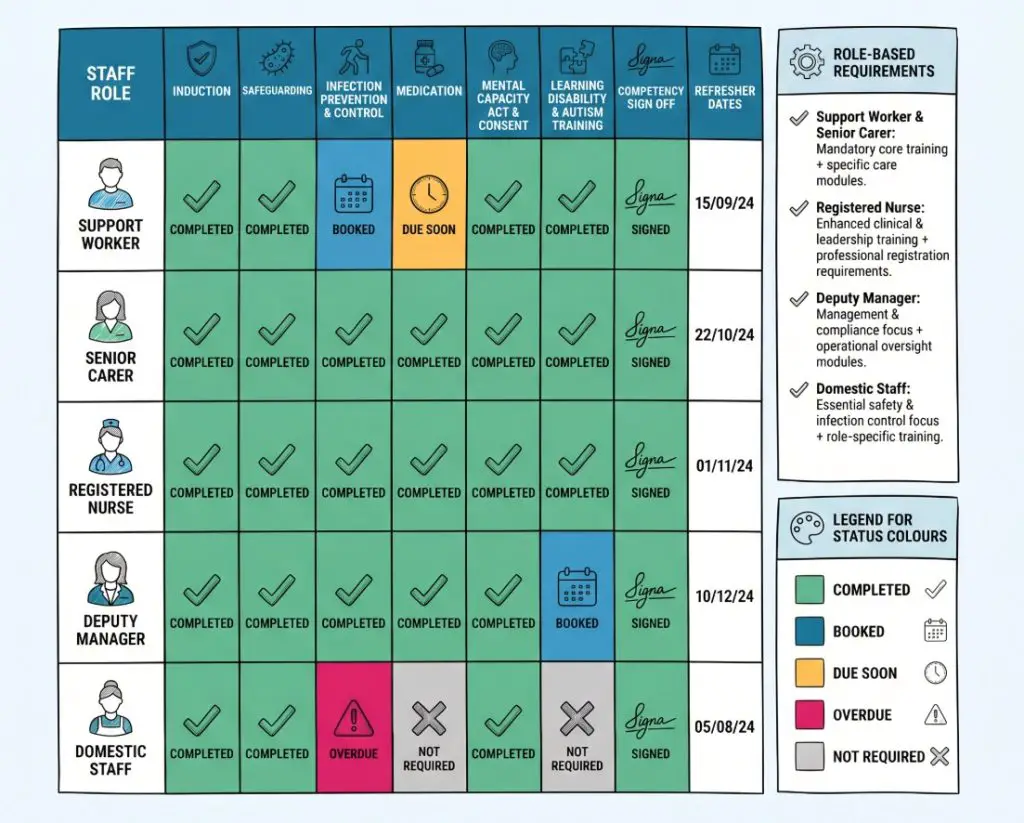
A training matrix is a working record of who needs which training, what has been completed, and when refreshers are due. It is usually set out as a grid. Staff names run down one side, training topics sit across the top, and each box shows a simple status such as completed, booked, due soon or overdue.
In health and social care, that grid does a lot of heavy lifting. It shows whether the workforce is ready for the work on the rota. A service can have sound policies and experienced staff, yet still leave gaps hidden if records sit in separate folders, email chains and spreadsheets. Messy records cause messy decisions.
A good matrix brings order to that picture. It helps a registered manager, deputy manager or team leader see who has finished induction, who still needs practical sign off, and who is due a refresher before a gap turns into a risk. Regulation 18 on staffing expects providers to give staff the support, training, supervision and appraisal they need. The CQC fundamental standards point in the same direction.
“A training matrix should show more than attendance. It should show readiness.”
At its best, the matrix answers one plain question. Are the people on duty trained for the care they are expected to give?
Why a Training Matrix Helps Care Quality
The value of a training matrix is practical. It reduces guesswork. In a care setting, guesswork causes trouble quickly. If nobody can say with confidence who is current on safeguarding, medication support or moving and assisting, managers start relying on memory. Memory is not a safe system.
A matrix makes gaps visible early. It can show that a new support worker still needs shadow shifts before lone working. It can flag that half the team are due an infection prevention refresher next month. It can show that only a few staff hold current training in epilepsy awareness, diabetes support or autism training. Once those gaps are visible, rotas, supervisions and training plans become easier to manage.
People receiving care feel the difference. A worker with the right learning and the right checks is more likely to support medicines safely, use equipment properly, keep records straight and notice changes in a person’s condition or behaviour. A worker who is unsure may still try to do a good job, but uncertainty often shows up in slower responses, missed details and uneven care.
This is where the matrix earns its place. Skills for Care guidance on statutory and mandatory training links training to role and risk. The Health and Safety Executive guidance on training also makes clear that staff need adequate training when they start work and when risks, systems or responsibilities change. SCIE’s work on workforce development adds another useful point: training is more effective when it connects to real care practice rather than sitting apart from it.
“When training records are scattered, the service is running on hope. A matrix replaces hope with a clear view.”
There is a staff benefit as well. New starters can see what comes first. Senior staff can see what sits behind extra responsibility. Supervision becomes more useful because it is grounded in facts rather than general impressions. Shorter conversations, better decisions.
What a Good Training Matrix Should Include
A useful matrix should be easy to read at a glance. It should also hold enough detail to support real decisions. At a minimum, it should include the staff member’s name, role, training topic, date completed, renewal date and current status.
Most services need a little more than that. A stronger matrix often includes the start date, whether the person is new to care, whether the topic is mandatory for that role, whether the learning was face to face or online, and whether a practical competency check is still outstanding. That last point is often missed.
Completion does not always mean competence. A worker may pass an online medication course and still need observed practice before administering medicines alone. The same applies to moving and assisting, hoist use, catheter care, delegated healthcare tasks and other practical duties. A familiar line from senior carers is, “green on the sheet doesn’t always mean ready on the floor”. That is blunt, but fair.
The Care Certificate standards are often part of the picture for new staff in support roles. The Mental Capacity Act Code of Practice shapes training needs where staff support decision making, consent and best interests. The Equality Act 2010 guidance is relevant too, especially where staff training needs to cover reasonable adjustments, accessible communication and fair treatment.
A simple layout often works well:
| Role | Core training | Role specific training | Competency check | Refreshers |
|---|---|---|---|---|
| Care worker | Safeguarding, infection prevention, fire safety, moving and assisting | Personal care, record keeping, communication | Yes, where tasks are practical | Yes |
| Senior carer | Core subjects plus medication, supervision, escalation | Delegated tasks, incident review | Yes | Yes |
| Registered nurse | Core subjects plus clinical requirements | Wound care, medicines, clinical observations | Yes | Yes |
| Domestic or ancillary staff | Health and safety, fire safety, safeguarding awareness | Cleaning standards, food safety if relevant | Sometimes | Yes |
Typical topics in a matrix may include:
- Safeguarding: Staff need to spot concerns, respond properly and report without delay. This links closely to the Care Act statutory guidance and local safeguarding procedures.
- Infection prevention and control: This supports safer personal care, cleaner equipment and safer shared spaces.
- Moving and assisting: Staff need safe techniques and, where used, safe handling of equipment such as hoists and slings.
- Medication support or administration: The level depends on the role and setting. NICE guidance on managing medicines in care homes and NICE guidance for home care show why this area needs clear systems.
- Health and safety: This may include fire safety, accident reporting, lone working and risk awareness.
- Mental Capacity Act and consent: Staff need a working grasp of decision making, capacity and lawful support.
- Learning disability and autism training: In England, the Oliver McGowan code of practice sets the standard for CQC registered providers and their staff.
“The best matrix is not the longest one. It is the one that matches the real work of the service.”
How the Matrix Should Be Organised by Role
A common mistake is giving every role the same training list. It looks tidy. It is rarely the best fit.
Different roles carry different duties. A support worker delivering personal care needs a different training profile from a domestic worker, receptionist, team leader, registered nurse or registered manager. The matrix should make those differences obvious. When it does not, the service ends up with too much generic learning and not enough role specific preparation.
A role based approach also keeps the matrix useful. Staff are less likely to be overloaded with irrelevant modules, and managers are less likely to miss specialist learning that a role genuinely needs. The structure stays cleaner too. Better still, it becomes easier to explain.
A practical way to separate roles looks like this:
- Care workers and support workers: These roles often need induction, safeguarding, infection prevention, communication, moving and assisting, record keeping and service specific learning linked to the people they support.
- Senior carers or senior support workers: These roles may need the core list plus medication, supervision, escalation, delegated tasks and stronger incident awareness.
- Registered nurses: These roles need core subjects, but also role specific clinical training and professional requirements.
- Registered managers and deputies: These roles often need leadership, governance, safer recruitment, audit, complaints handling and oversight of training systems.
- Ancillary staff: Domestic, kitchen, maintenance and driver roles may need a smaller set, but it still needs to match the duties and the environment.
There is an important point here. Fairness does not mean identical training for everyone. Fairness means each person gets the learning needed for the job they actually do. A domestic worker in a care home may need safeguarding awareness and infection prevention, but not the same moving and assisting training as staff who carry out transfers.
This role based structure also helps when agency and bank staff are used. Providers remain responsible for the care delivered on their behalf. Checks on training and competence cannot stop at the payroll boundary. A matrix that leaves temporary staff out is only telling half the story.
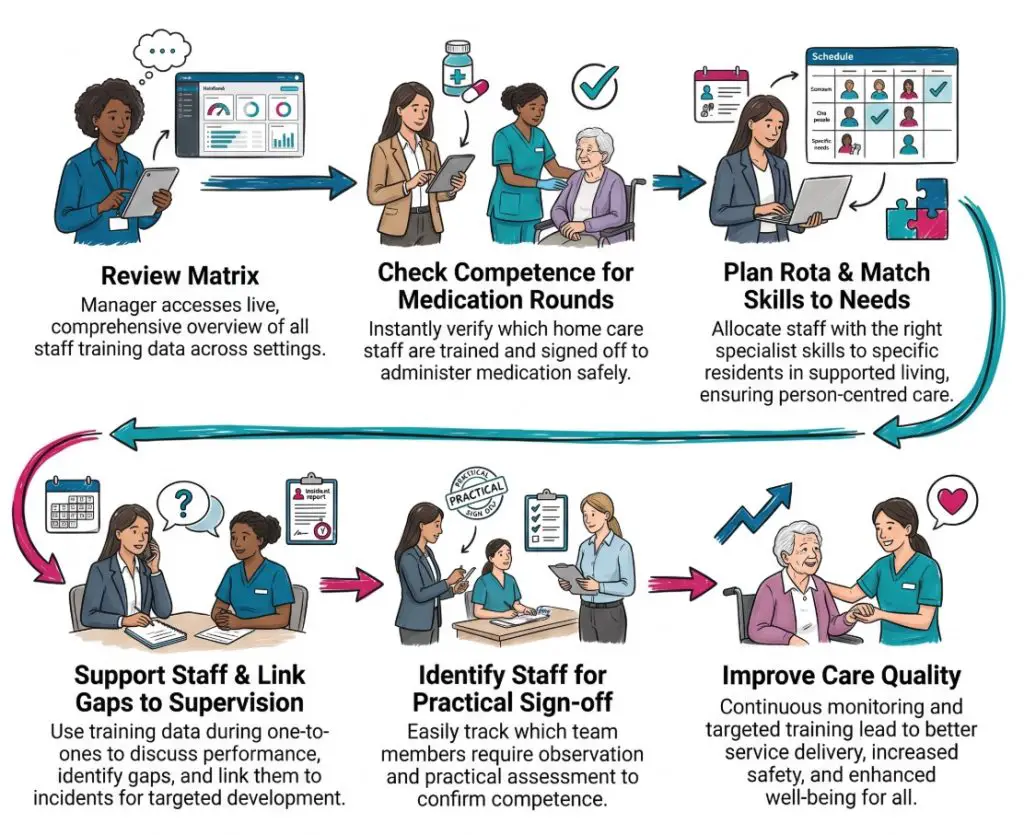
How a Training Matrix Works Day to Day
A matrix proves its worth on ordinary days. Not on inspection day alone.
Take a home care service. A new care worker has completed induction, safeguarding and infection prevention, but still needs lone working training and observed medication support. The matrix should show that clearly. The worker may be ready for shadowed visits and lower risk calls, but not for every task on every run.
Now look at a care home. Several staff are due moving and assisting refreshers next month. One senior carer is overdue for medication training. A new resident is moving in with diabetes and early dementia. The matrix helps the manager connect staff capability with the needs of the home. That may lead to refresher bookings, a temporary change to medication rounds, or extra supervision.
Supported living offers another picture. A service for autistic adults and people with a learning disability may need strong coverage in communication, sensory awareness, safeguarding and behaviour support. A day service may need a different blend, with more focus on activities, transport, community access and emergency response. The matrix should reflect the setting rather than flatten everything into one standard list.
Useful questions a matrix can answer quickly include:
- Who can cover medication rounds: This helps managers avoid unsafe assumptions when planning shifts.
- Who still needs practical sign off: Training may be complete, but the person may not yet be ready to work alone.
- Which refresher dates are coming up: This helps spread bookings rather than leaving several topics overdue at once.
- Are training gaps linked to recent incidents: A cluster of falls, documentation problems or medicines errors may point to a learning gap or a system issue.
- Does the team fit the people in the service: New needs in the service often mean the matrix needs updating too.
One home care worker might put it more simply: “I just need to know what I’m cleared for and what still needs checking”. That kind of comment comes up again and again because staff want clarity, not guesswork.
The matrix does not solve poor staffing on its own. It cannot create time, cover sickness or replace good supervision. Still, it gives managers a much clearer basis for decisions, and that alone can prevent avoidable problems.
When the Matrix Should Be Reviewed
The matrix should be reviewed at set points across the year. A matrix that sits untouched for months soon loses value.
Induction is the first clear point. New starters need a visible route through early learning. The matrix can show what should be completed before direct care, what should be covered during shadowing, and what needs sign off before independent work begins. For staff who are new to care, the Care Certificate often shapes that first stage.
Other useful review points include:
- During probation: This shows whether the new starter is moving through the expected training and whether more support is needed.
- At supervision and appraisal: Managers can link training records with observed practice, confidence and progress.
- When a role changes: A promotion or new duty often brings new training needs.
- After incidents or complaints: A review may show that refresher learning, coaching or a competency check is needed.
- When the service changes: New people, new equipment or new risks can change the training picture quickly.
- When law or standards change: The Oliver McGowan code of practice is a clear example of a change that affects what many providers must include.
A few managers see frequent review as an administrative burden that pulls time away from care. There is truth in that. Poorly designed systems do waste time. The answer is not to review less. The answer is to keep the matrix simple, current and tied to decisions that already need to be made.
Common Mistakes and How to Avoid Them
The biggest mistake is treating the matrix as proof of competence. It is proof that training has been recorded. That is not the same thing.
A second mistake is letting it drift out of date. Once managers stop trusting the matrix, they go back to folders, emails and memory checks. From there, oversight weakens quickly. Confidence drops as well.
Other common mistakes show up again and again:
- Using a generic template: A standard list may miss the needs of the actual service or include training that does not fit the role.
- Ignoring temporary staff: Bank and agency staff still need proper checks before taking on duties.
- Recording courses but not refreshers: A past completion date tells only half the story.
- Missing competency checks: Practical tasks need observation, not just certificates.
- Overloading new starters: Too many modules too soon can create a false sense of progress.
- Failing to link training with incidents: Learning plans should reflect what is happening in the service, not sit in a separate world.
Here is one typical example. A service marks all staff green for medication because they passed e learning. During supervision, two newer workers admit they are still unsure about MAR charts and covert medication processes. The matrix looks healthy, yet the real position is mixed. A stronger version would show course completion and competency sign off as separate items.
A neat spreadsheet can hide a messy truth. That is why managers need the matrix to be honest, not just tidy.
What Legislation, Standards and Bodies Are Most Relevant
Several parts of the legal and regulatory framework sit behind a training matrix in England. The clearest legal link is Regulation 18 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014. This covers staffing and includes support, training, professional development, supervision and appraisal.
Regulation 12 is also relevant because safe care and treatment depend on staff having the right skills and experience. The CQC fundamental standards bring these expectations together in a form providers recognise quickly.
The wider framework often includes:
- Skills for Care guidance: This helps providers identify statutory and mandatory training and build role based learning plans.
- The Care Certificate: This is widely used for people who are new to care and support roles.
- Health and Safety Executive guidance: This links training to starting work, changing risks and changing systems.
- The Mental Capacity Act 2005: This shapes training on consent, decision making and best interests.
- The Care Act 2014: This underpins adult safeguarding and wider care responsibilities.
- The Equality Act 2010: This supports training on fair treatment, accessibility and reasonable adjustments.
- SCIE resources: These can help services connect workforce learning with day to day care quality.
- The Oliver McGowan code of practice: This sets standards for learning disability and autism training for CQC registered providers and staff.
These frameworks do not mean every service should build the same matrix. They do mean a training matrix should be grounded in law, role, risk and the needs of the people receiving care. The legal meaning stays fixed. The way a service organises the matrix around that framework may vary.
Conclusion
A training matrix is a simple tool, yet it tells a service a great deal about itself.
Used badly, it becomes a checklist that gives false reassurance. Used well, it becomes a live record of workforce readiness. It shows what staff have completed, what still needs sign off, when refreshers are due and where the service may be exposed.
That is why the strongest matrices do more than store dates. They support safer deployment, clearer induction, better supervision and more focused quality checks. They help turn a pile of training records into something useful on the floor.
A sensible next step for any service is to look at its current matrix and ask three direct questions. Does it match real roles. Does it separate completion from competence. Does it help managers make safer decisions this week, not just pass an audit next month.
Practical checklist
- Role by role coverage: Each post should have a training list that fits the actual duties.
- Clear status labels: Completed, booked, due soon and overdue should be easy to spot.
- Competency checks: Practical duties should have a separate sign off where needed.
- Refreshers built in: Renewal dates should be visible and reviewed regularly.
- Service specific topics: The matrix should reflect the people who use the service.
- Temporary staff included: Agency and bank workers should not sit outside the system.
- Used in supervision: The matrix should support real conversations, not sit untouched.
- Linked to incidents: Repeated concerns should trigger a review of learning and competence.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.