
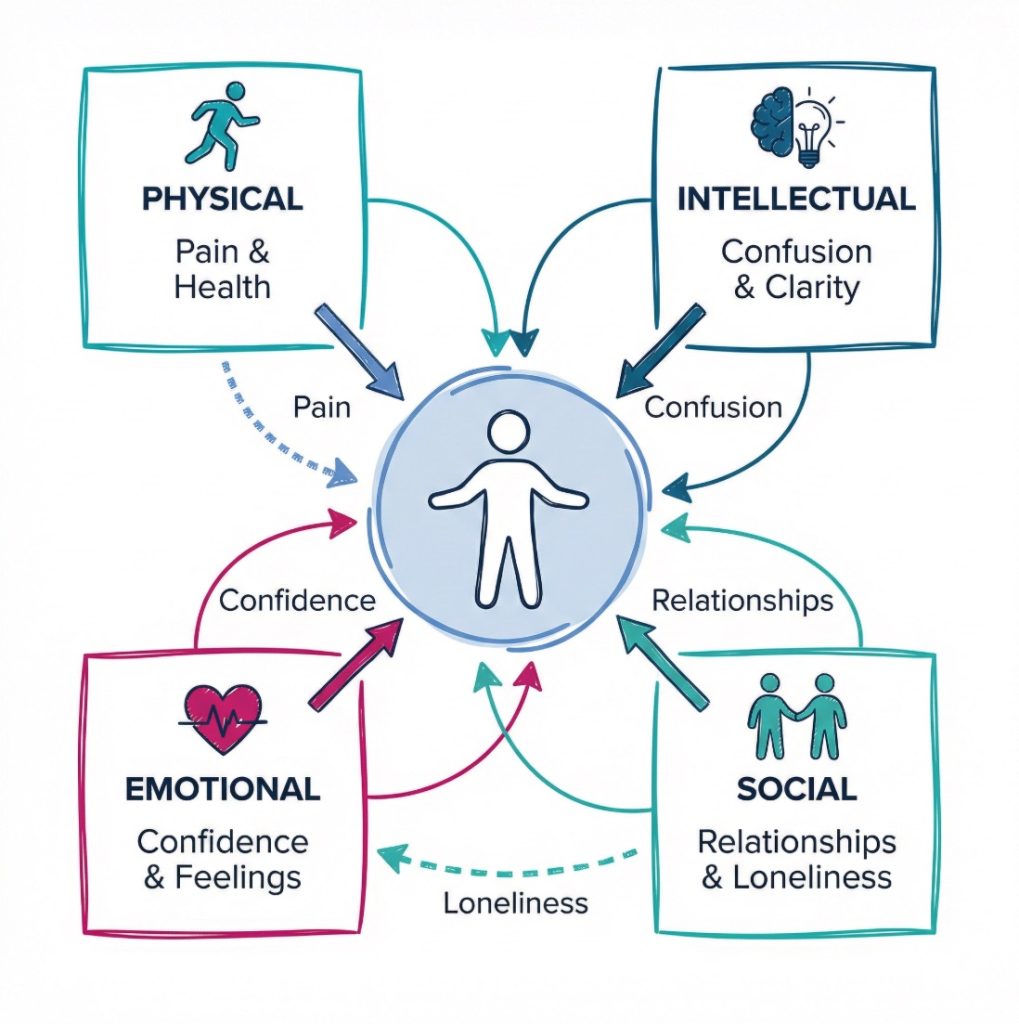
PIES stands for physical, intellectual, emotional and social development. In health and social care, it gives people a simple way to look at the whole person instead of reducing them to one need, one diagnosis or one event. It is often linked with a person centred approach to care, because people do not live in tidy boxes. Their body, thoughts, feelings and relationships keep affecting one another.
A person may have strong mobility but feel lonely. Someone else may be very sociable but struggle with memory or concentration. Another person may seem physically settled while carrying grief that changes appetite, sleep and confidence. PIES helps staff, learners and carers notice those links early. It also keeps attention on daily life, dignity and independence rather than tasks alone.
“PIES works best when it keeps the whole person in view, not just the part that looks most obvious.”
This is one reason the framework appears so often in care training. It is easy to remember, but it opens up a deeper way of thinking. The NHS guide to care and support and the wider NICE social care pages both reflect that broader view of wellbeing, support and quality of life. PIES fits neatly into that way of working.

The Physical Part of PIES
The physical part covers the body and how it functions day to day. That includes growth, movement, sleep, nutrition, continence, hygiene, pain, illness, medication, balance and the senses. In many care settings, this is the part people spot first because it is visible. Someone may lose weight, walk more slowly, become breathless or look unusually tired. Those signs can change what the person can do for themselves and how safe they feel.
Physical wellbeing shapes daily life in very practical ways. It affects whether someone can get up, wash, dress, eat, take part in activities or manage a short journey. Pain can make a person quieter or more irritable. Poor sleep can reduce concentration. A fall may lead to injury, but it can also lead to fear and loss of confidence. The NHS advice on falls shows how closely physical safety and independence are linked.
For staff, the physical part of PIES goes beyond spotting illness. It includes noticing patterns. A person who starts staying in their room may be in pain. A person who refuses meals may have swallowing problems, low mood or nausea. Physical support also involves dignity. Assistance with washing, continence or mobility can protect comfort, but the way that support is given affects self esteem as well.
A caveat here is that physical needs are not always the starting point, even when they are the most visible. A person may complain of tiredness when the deeper problem is worry, isolation or poor sleep after bereavement. Still, the physical signs often give the first clue that something has changed.
“A change in movement, sleep or appetite can be the first sign that more than one part of a person’s life is under strain.”
Useful signs to look for include the following:
- Mobility changes: A person may walk less, need more support or avoid stairs because they feel unsteady or sore.
- Appetite changes: Eating less, skipping meals or drinking poorly can affect strength, mood and concentration.
- Sleep problems: Broken sleep may leave the person confused, low in mood or less able to cope with the day.
- Pain or discomfort: Unexplained irritability or withdrawal can sometimes point to pain that has not been clearly described.
- Personal care difficulties: Trouble washing, dressing or toileting can reduce confidence and increase dependence.
The Intellectual Part of PIES
The intellectual part is about thinking, learning, memory, concentration, problem solving, communication and decision making. In some settings, people use the word cognition. That simply means the mental processes involved in taking in information, making sense of it and using it. This part of PIES is not only about formal education or academic ability. It is about how a person manages information in everyday life.
A person’s intellectual wellbeing can be shaped by age, disability, illness, medication, stress, fatigue, sensory loss or lack of stimulation. Someone who is bored and cut off from conversation may appear slower or less engaged over time. By contrast, a person who is offered choices, discussion and meaningful activity may stay involved for longer. This is one reason care plans often work better when they reflect the person’s routines, interests and preferred ways of communicating.
The NHS pages on dementia symptoms show that changes in memory, language and concentration can appear gradually and affect daily life in many ways. Yet intellectual needs are not limited to dementia. A person recovering from illness may struggle to focus. A person under stress may find decisions harder. A person with hearing loss may seem confused when they have simply missed part of the conversation.
For staff, this part of PIES often comes down to pace and clarity. Information may need to be broken into smaller parts. Questions may need more time. Records need to reflect how the person communicates best, and whether they need support with decisions. The Mental Capacity Act guidance for health and social care workers is relevant here because it sets out how decision making should be approached when someone may struggle to make some choices for themselves.
A common mistake is to treat confusion as refusal or silence as lack of interest. Sometimes the person has not processed what was said. Sometimes the environment is too noisy. Meanwhile, good communication can keep a person involved far longer than people expect.
- Memory: Forgetting names, times or steps in a routine can increase anxiety and reduce independence.
- Attention: Poor concentration may affect safety, conversation and the ability to follow a plan.
- Choice making: Some people need more time or simpler information to show what they want.
- Communication: The person may understand more than they can express, or express more than others first assume.
The Emotional Part of PIES
The emotional part covers feelings, mood, self image, confidence, attachment, resilience and the ability to cope with change. Emotional wellbeing does not mean being cheerful all the time. It is more about whether the person feels secure, valued and able to manage the pressures around them. In care settings, emotional wellbeing can affect almost everything else. Appetite, motivation, sleep, communication and behaviour can all shift when someone feels frightened, ashamed, lonely or low.
This part of PIES is often less visible than the physical part, but it can be just as powerful. A person may smile and still feel deeply anxious. Another may become angry when they are actually frightened. Grief, pain, trauma, sudden illness, loss of routine and dependence on others can all change how safe a person feels. The NHS advice on loneliness is useful here because loneliness is not only social. It can affect mood, confidence and health more broadly.
In daily care, emotional wellbeing is tied closely to dignity. Being rushed through personal care, being talked over, or being left out of decisions can wear a person down. Small moments count. A calm tone, a familiar face and time to respond can reduce distress more than people realise. The Care Certificate standard on working in a person centred way reflects that link between respect, communication and wellbeing.
Some people argue that emotional care is too vague to be measured properly. There is some truth in that. Feelings are personal, and not every sign is easy to interpret. Yet the counterpoint is stronger: when emotional distress is ignored, daily care usually becomes harder, not easier. Refusal, withdrawal and agitation often grow when fear or sadness has gone unnoticed.
“People rarely separate feelings from daily care. Fear, grief and shame can change how a person eats, sleeps, speaks and joins in.”
Examples of emotional signs include these:
- Low confidence: A person may stop trying tasks they could still manage with a little support.
- Anxiety: Restlessness, repeated questions or avoiding certain routines may reflect worry rather than defiance.
- Low mood: Tearfulness, poor appetite or loss of interest can affect the whole day.
- Emotional withdrawal: Quietness and reduced eye contact may signal distress, exhaustion or grief.
The Social Part of PIES
The social part is about relationships, belonging, communication, family, friendship, culture, faith, roles and community life. Social wellbeing looks different for each person. One person may want lively group activity. Another may prefer one trusted relationship and a quiet routine. PIES works well here because it avoids the idea that everyone should socialise in the same way.
Social needs can be overlooked when physical tasks dominate the day. Yet isolation can quickly affect mood, confidence and motivation. A person who stops seeing friends may become low in mood. A person who feels embarrassed about hearing loss may stop joining conversations. A person who moves into a new setting may lose old roles overnight. The NHS information on loneliness in older people shows how deeply connection and wellbeing are linked.
For the person receiving care, social wellbeing often comes down to feeling known. Being included in everyday talk, having contact with family, keeping links with culture or faith, and taking part in familiar routines can all protect identity. This is where Skills for Care guidance on person centred care is helpful, because it focuses on care that reflects the individual rather than the service timetable.
For staff, social care is often about removing barriers. Transport, hearing support, timing, confidence, fatigue and language can all get in the way. On second thought, “social” can sound too broad a label. In reality, it often comes down to very concrete things: who the person speaks to, whether they feel welcome, and whether they still have a place in ordinary life.
Useful examples include the following:
- Family contact: Regular contact may support identity, comfort and emotional stability.
- Friendships: One trusted friendship can reduce isolation and support confidence.
- Community links: Clubs, faith groups or local spaces may help a person feel part of something familiar.
- Communication access: Hearing aids, quiet spaces or extra time can make social contact possible again.
Why PIES Is So Important in Real Care Settings
PIES is useful because the four parts keep overlapping. A physical problem can affect mood. Emotional distress can affect sleep. Loneliness can reduce appetite. Poor concentration can increase the risk of falls or missed medication. Staff often see one part first, but good care depends on looking wider. The NHS social care and support guide and the Skills for Care workforce resources both point towards that broader, joined up way of working.
A simple example makes the point. An older adult has a fall. Physically, they may be bruised and less steady. Emotionally, they may become frightened of walking. Socially, they may stop going to shared meals. Intellectually, they may lose confidence in planning simple tasks. Soon the fall has changed far more than mobility. PIES gives staff a way to notice that chain reaction early.
Another example is grief. A bereaved person may start sleeping badly, eating less and avoiding company. Their concentration may drop. Staff who only notice the reduced appetite may miss the rest of the picture. By contrast, staff who use PIES are more likely to record patterns, talk with the person and adjust support in a way that feels humane.
A short comparison can help:
| Part of PIES | What staff may notice first | Possible knock on effect |
|---|---|---|
| Physical | Falls, pain, tiredness, weight loss | Fear, withdrawal, less activity |
| Intellectual | Confusion, memory lapses, poor concentration | Unsafe choices, frustration, loss of confidence |
| Emotional | Tearfulness, anxiety, anger, low mood | Sleep problems, reduced appetite, social withdrawal |
| Social | Isolation, fewer visitors, less engagement | Low mood, poorer stimulation, reduced motivation |
“PIES is not a checklist for ticking boxes. It is a way to spot how one difficulty can spread across a person’s whole day.”
How to Think About PIES in a Person Centred Way
PIES works best when it stays flexible. It should support observation and conversation, not replace them. Two people with the same diagnosis may have very different strengths, worries and routines. One may value privacy above all else. Another may need regular contact and reassurance. A person centred approach in health and care starts with the individual, then uses frameworks like PIES to organise what has been noticed.
This also means looking for strengths, not only difficulties. A person may have limited mobility and still show humour, patience and strong relationships. Someone else may struggle with memory but respond well to routine, music or familiar conversation. Good care usually becomes more effective when staff recognise what still supports the person, rather than focusing only on loss.
There is also room for careful review. Needs can shift quickly after illness, bereavement, discharge from hospital or a change of setting. The NHS page on getting a care needs assessment shows how support is often built around what the person can do, what they find difficult and what outcomes they want. That fits well with PIES.
A practical checklist may help when reading a person’s situation through this lens:
- Physical needs: Changes in mobility, sleep, pain, appetite or personal care are recorded clearly.
- Intellectual needs: The person’s memory, concentration, communication and decision making are considered.
- Emotional needs: Mood, confidence, distress and coping are noticed rather than brushed aside.
- Social needs: Relationships, culture, belonging and routine contact are included.
- Strengths: Existing abilities, preferences and supportive relationships are recognised.
- Review: Changes over time are picked up, not treated as one off events.
Common mistakes also appear again and again:
- Focusing on one need only: Staff may respond to the obvious problem and miss the wider effect on daily life.
- Making assumptions: Quietness may be mistaken for calm, when the person is actually low in mood or confused.
- Treating social needs as optional: Isolation can quickly affect confidence, mood and physical health.
- Forgetting strengths: Support can become too task led if the person’s abilities and preferences are ignored.
Conclusion and Next Step
PIES gives health and social care a clear way to look at the whole person. The physical, intellectual, emotional and social parts are closely linked, and changes in one area often show up somewhere else. That is why the framework remains useful in care homes, hospitals, schools, supported living and community services. It helps explain what holistic care looks like in ordinary, practical terms.
Used well, PIES can lead to better observation, more accurate care planning and more respectful support. It can also remind staff and learners that people do not experience care in separate compartments. A person feels the quality of support through their body, thoughts, feelings and relationships all at once. Simple, but powerful.
The next step for many readers is to look at one real care situation and map it across all four parts of PIES. That often shows gaps, strengths and risks much more clearly than a single issue viewed on its own.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.