
Fit and proper staff are workers who are safe, suitable and able to carry out their role in health and social care. In England, this sits mainly within Regulation 19 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014. The rule says staff should be of good character, have the qualifications, competence, skills and experience needed for the work, and be physically and mentally able to do it, with reasonable adjustments taken into account.
This reaches far beyond a decent interview or a polished CV. A service should be able to show that a worker is suitable for the exact role they hold and safe to work with people who may be frail, unwell, distressed or dependent on support. Recruitment checks are part of that picture. So are induction, probation, supervision and day to day oversight.
Care work runs on trust. Staff may help with washing, dressing, eating, medicines, mobility, communication or safeguarding concerns. A poor appointment can show itself quickly. Rough care. Poor boundaries. Weak records. Unsafe decisions.
CQC places Regulation 19 within its wider guidance for providers and managers, while Skills for Care treats safer employment as a process that runs from recruitment through to managing leavers. Those two strands fit together. One covers the legal standard. The other shows how a service should live it out.
“Fit and proper staff” is not a label on a file. It is the difference between safe care and avoidable risk.
That is why this keeps appearing in inspections, safeguarding work and workforce guidance. It is not only an employment issue. It sits inside safe care, staffing, governance and public trust. Services that recruit carefully are usually steadier on the floor as well. The groundwork shows.
What does “fit and proper” mean?
The phrase brings together four connected ideas. Character comes first. A worker should be honest, respectful, reliable and safe in how they behave. Care roles often involve private spaces, personal information and an uneven balance of power. A person who is aggressive, manipulative, careless with boundaries or dishonest is not suitable for care work, whatever experience they bring.
Competence comes next. The worker should have the knowledge, skills and experience needed for the role they are actually doing. This does not mean every new starter must know everything on day one. It does mean the service should match the person to the role properly and keep them within safe limits while they learn. A new support worker may be right for an entry level post with close oversight, yet not ready to lead a shift or manage medicines alone.
Capability also sits inside the rule. Regulation 19 refers to workers being physically and mentally able to carry out the work, with reasonable adjustments considered. That point is often handled badly. A health condition or disability does not make someone unsuitable by itself. The proper question is whether they can do the job safely, with support or adjustments where needed. The Equality Act 2010 and the government’s guidance on reasonable adjustments for workers with disabilities or health conditions are part of that picture.
Then there is evidence. The provider should hold the recruitment information listed in Schedule 3, such as proof of identity, employment history and references. A service should be able to show why it decided a person was suitable. Good intentions do not fill gaps in a recruitment file.
- Character: The person should behave in a way that supports trust and safety. This helps protect people from abuse, neglect and exploitation.
- Competence: The person should know enough, and be supported enough, to do the role safely. This reduces avoidable mistakes.
- Checks: The service should gather and keep proper recruitment evidence. This shows the appointment was made with care.
- Capability: The person should be able to carry out the work safely, with reasonable adjustments where needed. This supports both safety and fairness.
On second thought, the word “fit” can mislead people here. It sounds fixed and absolute. It is not. Suitability depends on the role, the setting and the level of support around the worker. Someone may be fit for one post and not another.

Why fit and proper staff shape safe care
This rule exists to protect people who use services. In health and social care, people may rely on staff at the hardest points in daily life. Illness, frailty, confusion, pain and distress can make a small lapse feel much bigger. A poor recruitment decision can affect safety, dignity and trust in a very direct way. CQC’s guidance for providers and managers places Regulation 19 within the wider safety framework for regulated services.
Dignity sits in the middle of this. Two workers may complete the same task, yet the experience can be entirely different. One explains what is happening, protects privacy and notices discomfort. Another rushes, talks over the person and ignores the mood of the room. The task is done, yet the care is poor. SCIE’s guidance on dignity in care and communication reflects the same point. Privacy, tone and respect are part of safe care, not a soft extra.
The effect spreads through the whole service. One unsuitable worker can unsettle families, leave colleagues clearing up mistakes and weaken the tone of the team. Rushed recruitment often creates more pressure later because weak appointments bring more supervision, more complaints and more turnover. That pattern is familiar in care settings.
A carer in one CQC account described good support in simple terms: staff kept her informed and shared what she needed to know. That sounds basic. It is not. Clear, respectful communication usually sits beside careful recruitment and steady supervision.
Safe recruitment protects people before any care is delivered.
A fair objection is that a complete file does not guarantee good care. That is true. A tidy folder can still sit beside weak leadership or poor supervision. The answer is not to treat recruitment as secondary. It is to recognise that recruitment and daily management work together. Remove either one and the service is exposed.
Which law, regulation and bodies are linked to this topic?
The main legal source is Regulation 19. This is the rule most people mean when they talk about fit and proper staff in regulated services. It sets out the core requirements around character, competence and ability to carry out the work. It also links to Schedule 3, which covers the recruitment information a provider should have for each person employed.
The main regulator for regulated health and social care services in England is the Care Quality Commission. CQC’s guidance places Regulation 19 alongside staffing, safe care and treatment, and staff support. Its enforcement pages also show that action can follow when providers fail to meet this regulation.
The Disclosure and Barring Service is closely tied to the topic. Employers can request different levels of DBS check depending on the role. For work that counts as regulated activity with adults, an Enhanced DBS check with an Adults’ Barred List check may be available. Eligibility depends on the duties of the post, not the job title alone. The DBS workforce guidance helps explain the distinction.
Other parts of the legal framework sit nearby. The Care Act 2014 provides the wider safeguarding framework for adults with care and support needs. SCIE’s Care Act safeguarding resource is useful here because it shows how safe systems, professional curiosity and early action connect with adult safeguarding. The Mental Capacity Act 2005 and the Mental Capacity Act Code of Practice also have a place. Staff who support people who may lack capacity need sound judgement, respect for legal safeguards and the confidence to work within proper decision making processes.
Professional regulators shape the daily standards expected of staff as well. Nurses, midwives and nursing associates work to the NMC Code. Allied health professionals such as occupational therapists and physiotherapists may be regulated by the HCPC standards of conduct, performance and ethics. Social workers in England are regulated by Social Work England’s professional standards. These standards do not replace Regulation 19, though they show what safe conduct, competence and professionalism look like in day to day work.
The training side is there too. The Care Certificate standards set out the knowledge, skills and behaviours expected of new workers in health and social care. That does not prove someone is competent in every task. It does provide a baseline for induction, supervision and early development.
How providers check whether staff are fit and proper
The process usually starts before the job is advertised. The provider should be clear about the role, the level of responsibility and whether the work counts as regulated activity. Skills for Care’s safer employment guidance begins with planning for good reason. A vague role leads to vague decisions.
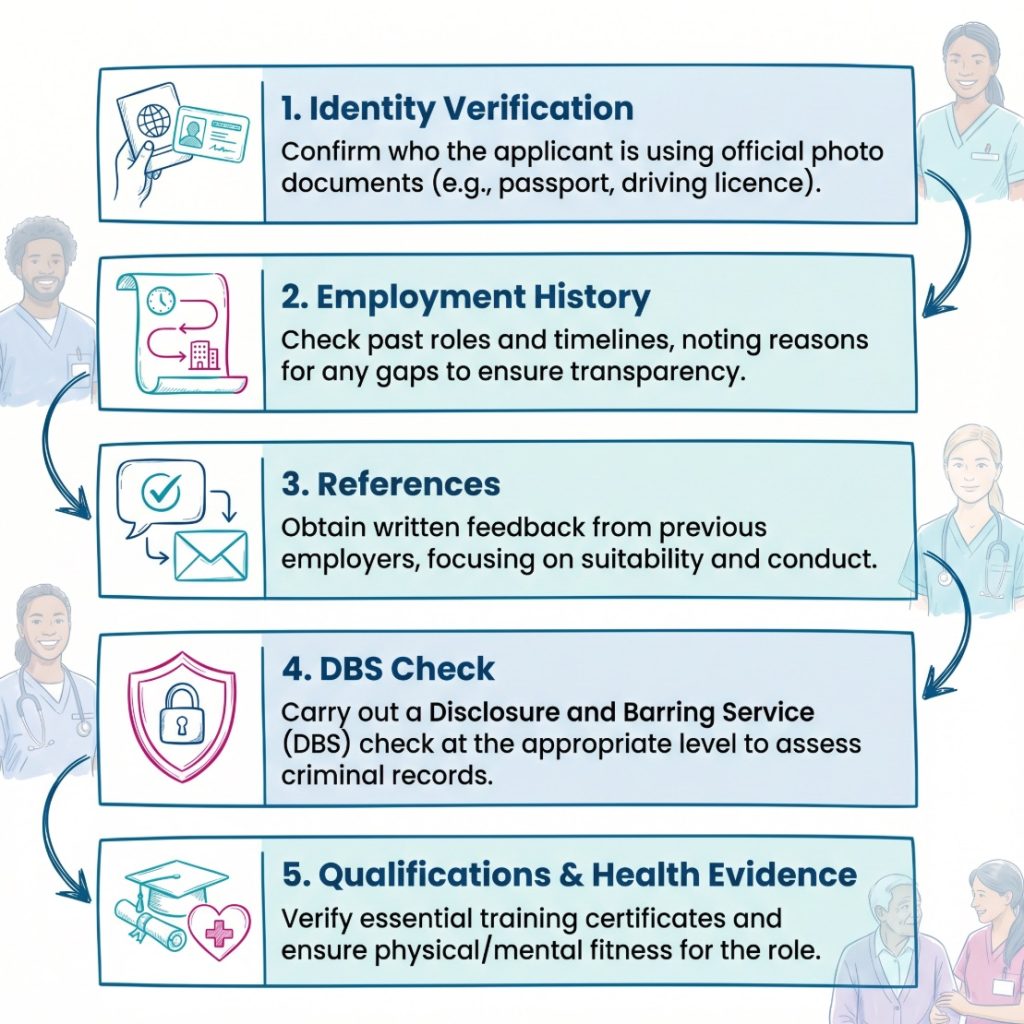
Next comes evidence gathering. This often includes proof of identity, a full employment history, references, relevant qualifications, professional registration where required and DBS checks where the law allows them. Skills for Care’s recruitment and vetting guidance talks about a curious safeguarding mindset. In plain terms, that means following up gaps, querying vague answers and looking at the whole picture rather than ticking boxes.
References deserve special attention. A short reference that confirms only dates adds very little. A fuller one can show whether there were concerns about conduct, attendance, boundaries or performance. That can be especially useful in care work, where behaviour and judgement often tell more than certificates do.
DBS checks are important, yet they are only part of the story. Government guidance explains when standard or enhanced checks are available and when barred list checks apply. A clear certificate does not prove a person is suitable in every respect. It is one piece of evidence. No more.
| Check or stage | What it looks for | Why it helps |
|---|---|---|
| Identity | Confirms the person is who they claim to be | Reduces the risk of fraud and hidden history |
| Employment history | Shows experience, gaps and patterns | Helps the provider spot issues that need follow up |
| References | Gives background on conduct and reliability | Adds context that CVs and interviews may miss |
| Qualifications and registration | Confirms training and legal status where needed | Supports safe role matching |
| DBS where eligible | Shows relevant criminal record information and barred list status | Adds a safeguarding layer for certain posts |
| Induction and probation | Tests how the worker performs in real settings | Shows whether the appointment is safe in practice |
A step by step view helps:
- Define the role: The service should know what the worker will do, what risks come with the post and what level of support is needed.
- Verify identity and work history: This confirms who the person is and whether gaps or patterns need explanation.
- Seek useful references: References should help the employer judge conduct and suitability, not just employment dates.
- Check qualifications and registration: This is especially relevant for regulated professional roles.
- Use the correct DBS route: The level of check depends on the duties attached to the role.
- Consider health and reasonable adjustments: The focus stays on safe practice and fair treatment.
- Use induction and probation properly: Observation, supervision and feedback show whether the person is safe in the role.
Where this shows up in different care settings
In a care home, fit and proper staff can often be seen in the smallest details. A worker may have the right documents and a clear recruitment file, yet managers still need to watch how they approach personal care, whether they respect residents and whether they know when to ask for help. A warm interview style is not enough. Real suitability appears in the daily handling of care.
A worker quoted in one inspection account spoke about staff taking time to reflect after incidents and speak properly with people. Paraphrased, the point was simple: good care is not rushed, and staff need space to think as well as do. That is a useful description of what safe teams look like.
In domiciliary care, the issue is often sharper because staff work alone in people’s homes. There may be far less direct supervision during the visit itself. That makes trust, punctuality, boundaries and record keeping especially important. A worker may be experienced, but repeated lateness, poor notes or casual shortcuts can make them unsuitable for lone working.
Hospitals add another layer because both registered and unregistered staff work side by side. A nurse should hold the right registration and work within the NMC Code. A healthcare support worker may not be regulated in the same way, but still needs safe recruitment, training and oversight. Here, suitability often shows itself in escalation, observation, record keeping and staying within one’s competence. In more physical areas of care, this also links to HSE guidance on moving and handling in health and social care, because unsafe practice can harm staff and the people they support.
Supported living brings its own risks. Staff may help with money, shopping, tenancy issues, medicines and access to the community. That creates a strong need for honesty and professional boundaries. A worker who borrows money, becomes over involved or ignores the support plan may raise serious concerns about suitability, despite appearing friendly and helpful.
A worker can look suitable on paper and still be unsafe in the setting where they actually work.
A few realistic examples show how this can play out:
- Care home example: A new care assistant has the right checks, but during induction they rush intimate care and speak sharply to residents. The concern lies in behaviour and values, not missing documents.
- Home care example: A domiciliary carer is experienced and kind, yet their notes are vague and families report missed routines. This points to a suitability issue because home care relies heavily on dependable practice.
- Hospital example: A support worker spots that a patient looks unwell but says nothing because they are unsure. This suggests a gap in competence or confidence that needs addressing before more responsibility is given.
- Supported living example: A worker starts treating a person’s spending money too casually and blurs social boundaries. That may signal risk even if daily tasks are completed.
When a worker is fit and proper, and when concerns can arise
A worker is not labelled fit and proper once and then left alone forever. The provider makes an initial judgement at recruitment, yet that judgement continues through induction, probation, supervision and later review. Skills for Care’s safer employment model reflects that wider approach, covering recruitment, management of concerns and the handling of leavers.
This is useful because some workers are suitable for appointment but still need time and support before they are fully confident. A new care worker may have the right values and a sound recruitment file, but still need close oversight for moving and handling, safeguarding records or medicines awareness. The issue is not whether they can be employed at all. The issue is whether they have been placed in a role with sensible limits and proper support.
Concerns may arise later for different reasons. Sometimes the issue is conduct, such as dishonesty, unsafe boundaries, aggression or repeated lateness that affects care. Sometimes it is competence, such as poor medicines practice, weak infection prevention or careless records. Health changes may also mean duties need review and adjustments. Good services pick up patterns early. They do not wait for serious harm.
This can also touch legal frameworks beyond recruitment. If a worker is supporting someone who may lack capacity, weak judgement can affect decisions that should sit within the Mental Capacity Act Code of Practice. If the worker is handling risk badly in a physical care task, the issue may overlap with HSE expectations on moving and handling risk assessment. Suitability is not sealed at appointment. It is tested by the work itself.
A simple timeline looks like this:
- Before employment: Suitability is assessed through checks, references, role matching and interview decisions.
- During induction: The service sees how the worker behaves in real situations and whether early support is enough.
- During probation: Managers can spot concerns while the person is still new to the role.
- During employment: Supervision, training, registration checks and safeguarding processes show whether the worker remains suitable.
What are the common mistakes and misunderstandings?
One common mistake is to assume that a DBS check settles everything. It does not. Government guidance is clear about eligibility and barred list checks, yet a certificate cannot show whether a person is honest, respectful or dependable in daily care. A clear DBS result and a poor worker can exist side by side.
Another mistake is to treat fit and proper staff as a paperwork exercise. A complete file can still sit beside poor induction, weak supervision or a team culture that ignores early warning signs. Safer employment guidance is helpful here because it connects recruitment to what happens after the contract is signed. That link is often where services slip.
There is also confusion between fit and proper staff and fit and proper directors. These are separate rules. Regulation 19 deals with staff employed for regulated activities. The director level requirement sits elsewhere in the legal framework. Mixing them together can cloud basic questions about a worker’s suitability for a frontline role.
A further misunderstanding is that suitability is absolute. It is not. Someone may be safe in one role and unsafe in another. Experience does not erase the need for oversight, and a good interview does not override weak references or worrying gaps in employment history. Services need a rounded view rather than a simple yes or no answer.
Common practice errors include:
- Ignoring employment gaps: A gap may be harmless, but it still needs to be explained and recorded.
- Accepting weak references: Date only references may miss conduct issues that are highly relevant in care roles.
- Rushing recruitment: Staffing pressure can lead to shortcuts, which increases risk for people using the service.
- Leaving new staff unsupported: A good appointment can still become unsafe if the person is expected to cope alone too early.
- Ignoring low level concerns: Small issues with boundaries, records or attitude can point to larger problems later on.
Safe care rarely fails in one dramatic moment. It often slips through small unchecked decisions.
Conclusion
Fit and proper staff are workers who are safe, suitable and able to do the role they have been employed to do. The idea includes character, competence, recruitment checks, capability, reasonable adjustments and the quality of support after appointment. It is a legal requirement, but it is also a plain test of whether a service takes safe care seriously.
The strongest view of the topic sits between law and daily care. Providers need careful recruitment, sound records, sensible role matching and close follow up once the person starts. Families and people using services feel the difference when those pieces are done properly. Staff benefit too, because safer recruitment often leads to clearer expectations, steadier teams and better support.
A short checklist brings it together:
- Right person: The worker has the character and values needed for care.
- Right role: The person’s skills and experience match the tasks they will do.
- Right checks: Identity, references, history and DBS processes are completed properly.
- Right support: Induction, probation and supervision test whether the role remains safe.
- Right review: Concerns are noticed early and dealt with before risk grows.
Subscribe to Newsletter
Get the latest news and updates from Care Learning and be first to know about our free courses when they launch.